The Common Vein:
Principles of Structure
Ashley Davidoff MD
Parts
Size
Shape
Position
Character
Time
Common Terms
| Word First | Definition |
|---|---|
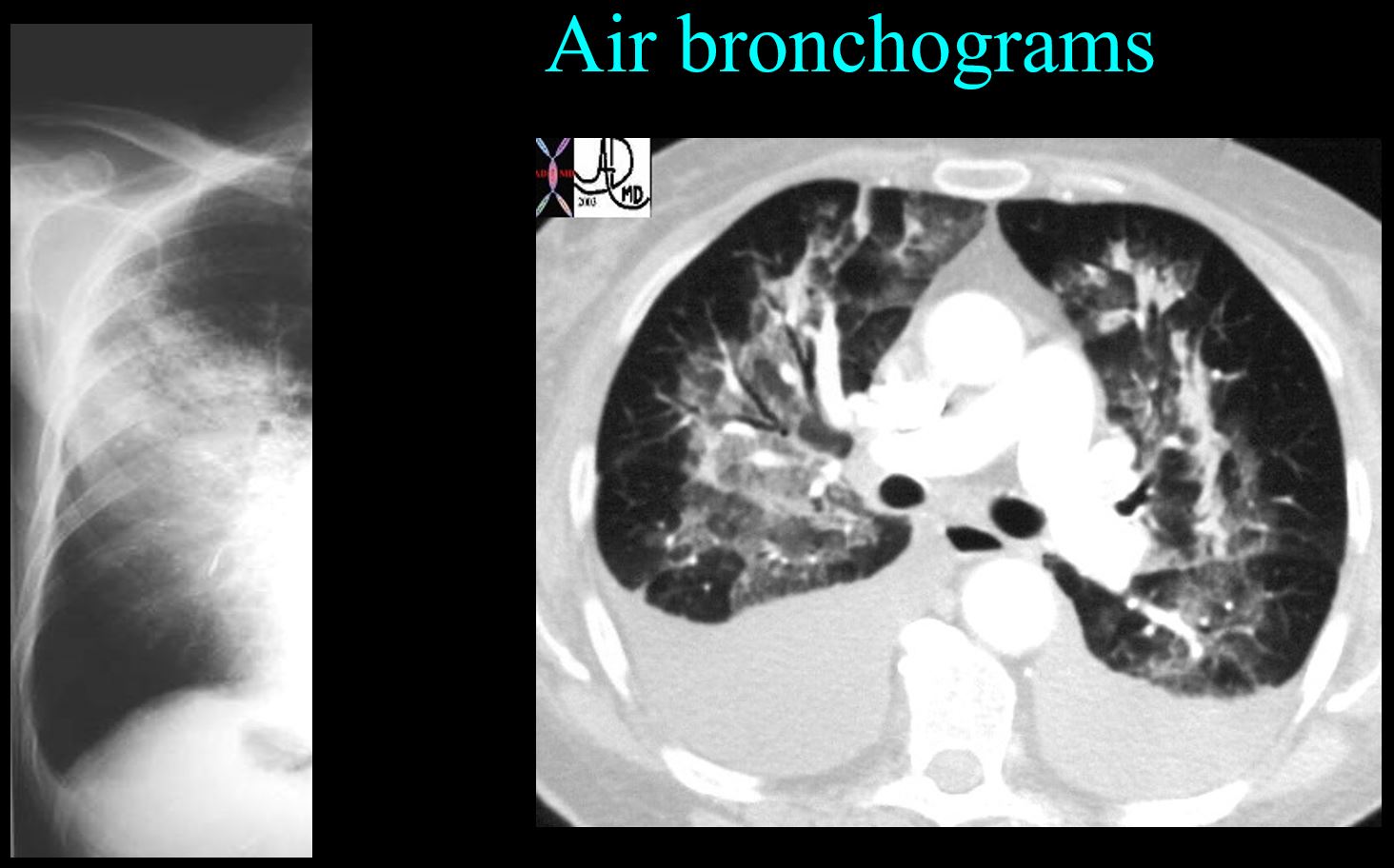
| air bronchogram | |
| atelectasis | |
| bleb | |
| bronchiectasis | |
| bulla | |
| congestive heart failure (CHF) | |
| consolidation | |
| effusion pleural (small, large, subpulmonic, decubitus films, supine and upright) | |
| ground glass opacity (GGO) | |
| mass solid lung mass | |
| nodule solitary pulmonary (spn) | |
| pneumothorax | |
| pneumothorax tension | |
| silhouette sign | |
| white out opacification distinguishing causes of hemithorax (effusion, vs vs pneumonia vs pneumonectomy) |
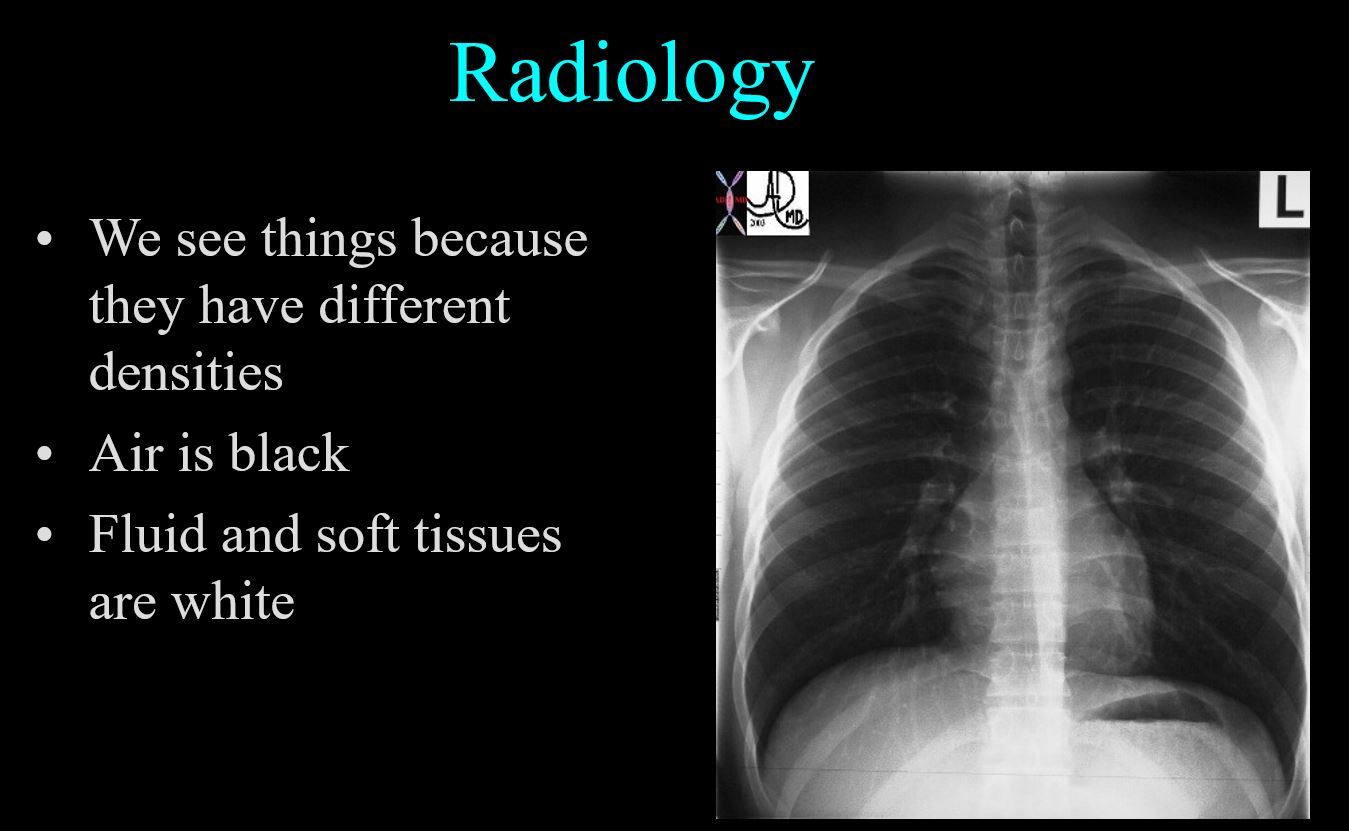
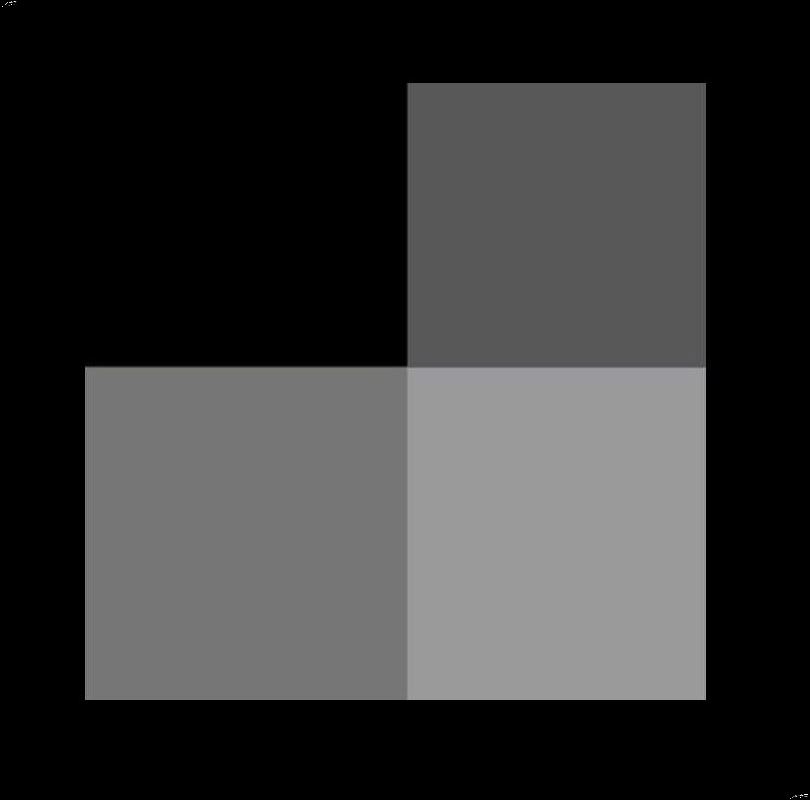
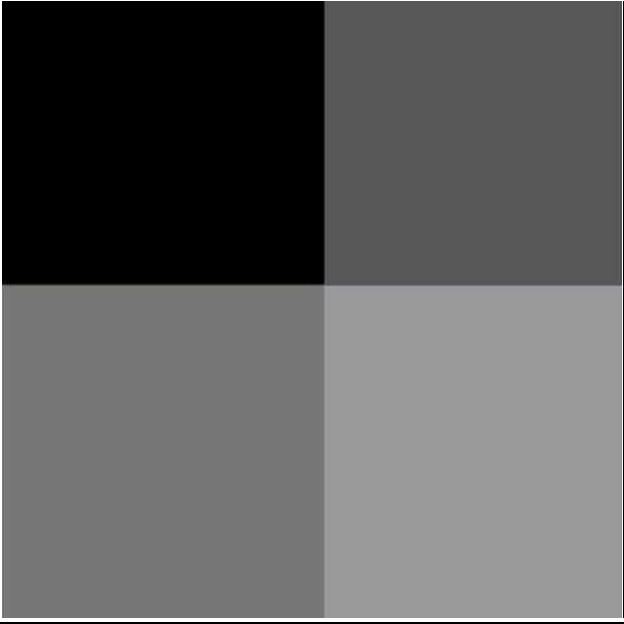
Why We See Things?
Ashley Davidoff thecommonvein.net
Ashley Davidoff thecommonvein.net
Ashley Davidoff thecommonvein.net
Silhouetting
Source
Signs in Thoracic Imaging
Journal of Thoracic Imaging 21(1):76-90, March 2006.
Ashley Davidoff thecommonvein.net
How to Approach the Field of Radiology
My Story – Curiosity
-
Sherlock Holmes
Not invisible but unnoticed Watson….
Ashley Davidoff thecommonvein.net
In the Pursuit of Excellence
In the pursuit of excellence of piano playing … principles are
Notes Scales and Music
-
-
THE ART OF PERFECTING MUSIC
Ashley Davidoff
Scales from MusicNotes.com
thecommonvein.net
-
-
THE ART OF PERFECTING DANCE
Ashley Davidoff
thecommonvein.net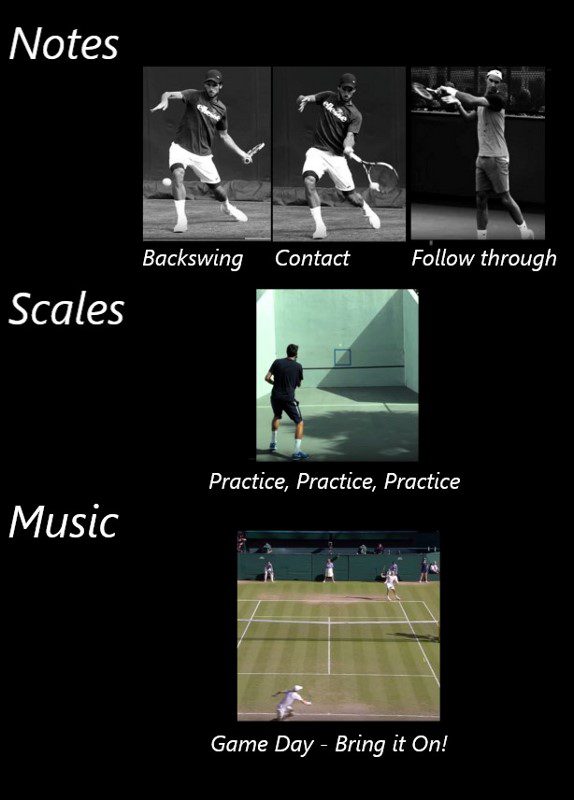
THE ART OF PERFECTING TENNIS
Ashley Davidoff
thecommonvein.net
TIGER WOODS AND TOM BRADY
NOTES SCALES AND MUSIC IN THE PURSUIT OF PERFECTION
Both images are in the public domain
Story of Dr Jerry Balikian
Application to Radiology
-
-
- Where to look, how to look and
-
- what to look for
- Ashley Davidoff thecommonvein.net
-
Notes
Anatomy of the Lungs
Frontal Examination of the Lungs

Ashley Davidoff MD
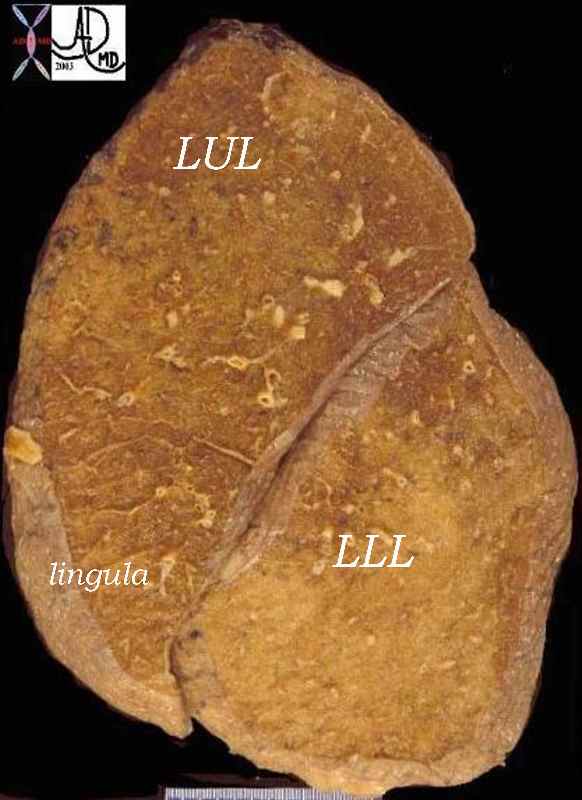
Parts of the Lungs- Basics
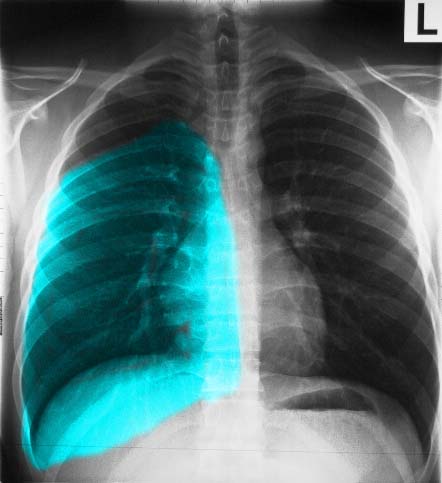
Left Lung – Left Upper Lobe – Frontal Projection
Ashley Davidoff MD
Frontal Projection Left Lower Lobe

Ashley Davidoff MD
Right Lung – Right Upper Lobe – Frontal Projection
Ashley Davidoff MD
Right Middle Lobe – Frontal Projection
Ashley Davidoff MD
Right Lower Lobe – Frontal Projection
Ashley Davidoff MD
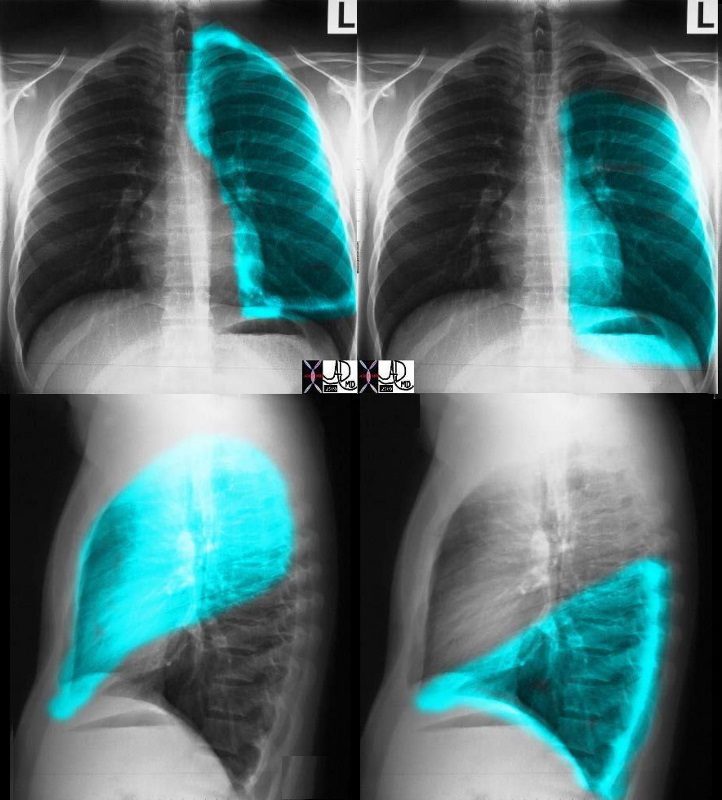
Lateral Examination of the Lungs
Major Fissure on the Left
Ashley Davidoff MD
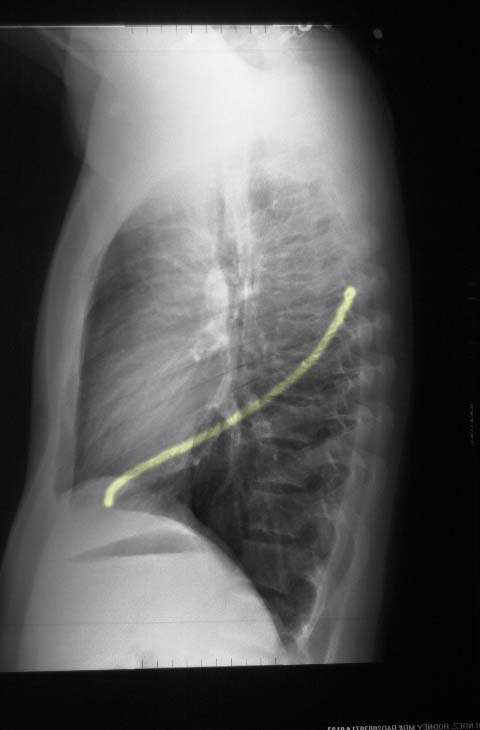
Ashley Davidoff MD
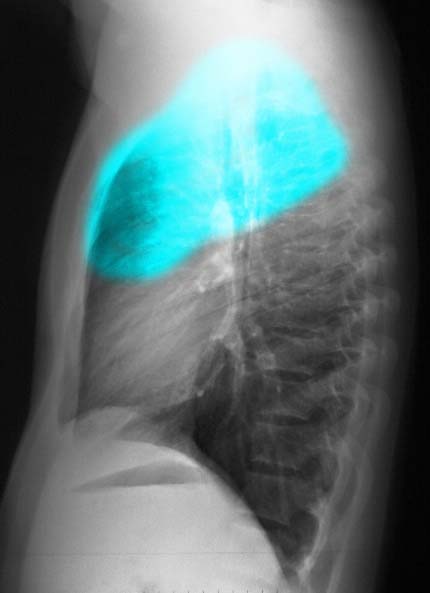
Lateral Projection – Left Upper Lobe
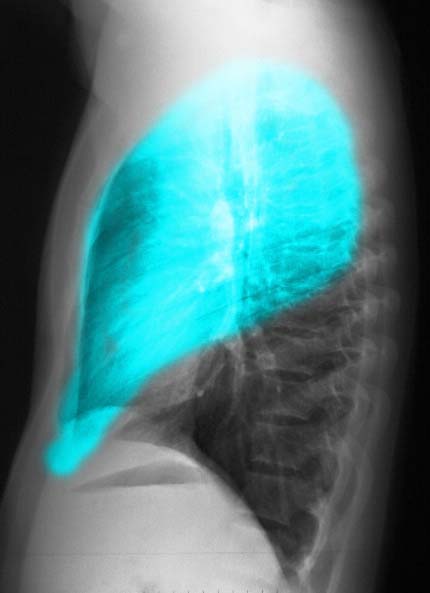
Ashley Davidoff MD
Lateral Projection left Lower Lobe
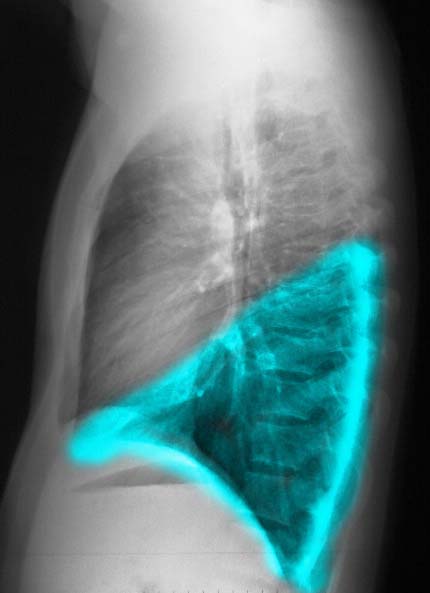
Ashley Davidoff MD
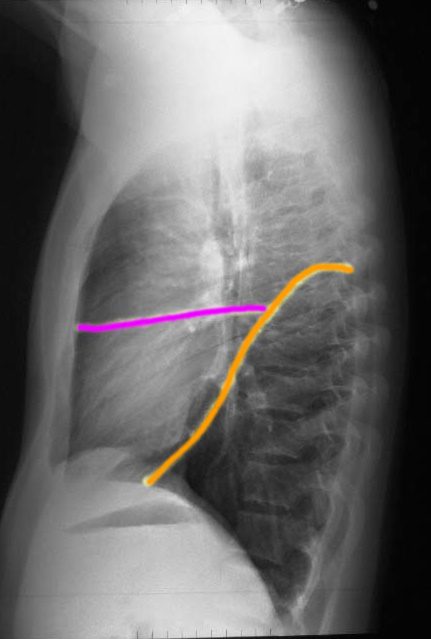
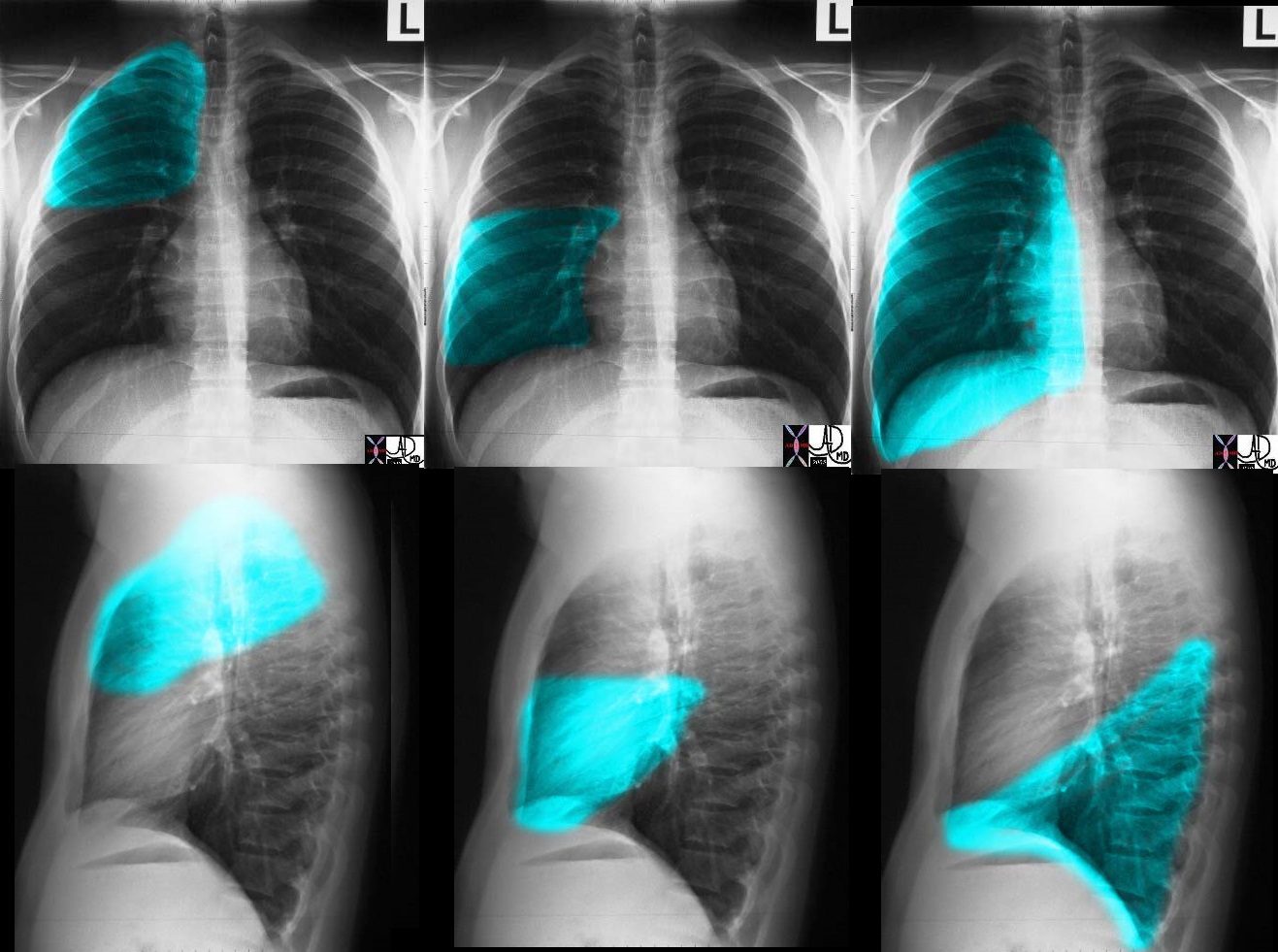
Major and Minor Fissures on the Right

The right lung has a small right upper lobe (RUL) separated from the middle lobe (RML) by the minor fissure (pink,lower image) . Both the RUL and RML are anterior and are separated from the lower lobe by the major fissure (orange line)
Ashley Davidoff MD
The right lung has a relatively small right upper lobe (RUL) separated from the middle lobe (RML) by the minor fissure (pink,lower image). Both the RUL and RML are anterior and are separated from the lower lobe by the major fissure (orange line)
Ashley Davidoff MD
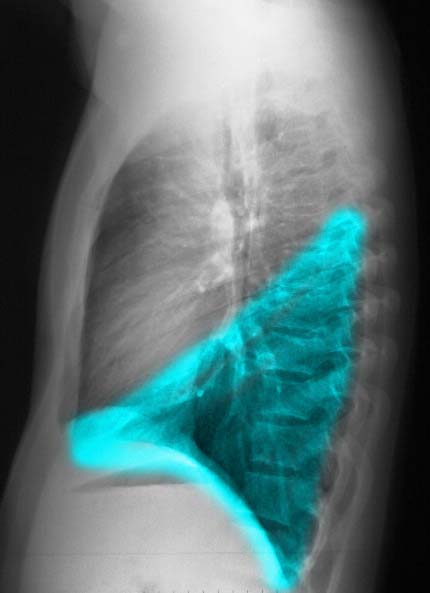
Right Upper Lobe – Lateral Projection
Ashley Davidoff MD
Right Middle Lobe – Lateral Projection

Ashley Davidoff MD
Right Lower Lobe – Lateral Projection
Ashley Davidoff MD
Summary
CXR of LEFT LUNG
Ashley Davidoff MD
Ashley Davidoff MD
Trachea, Main Stem Bronchi, and Carina
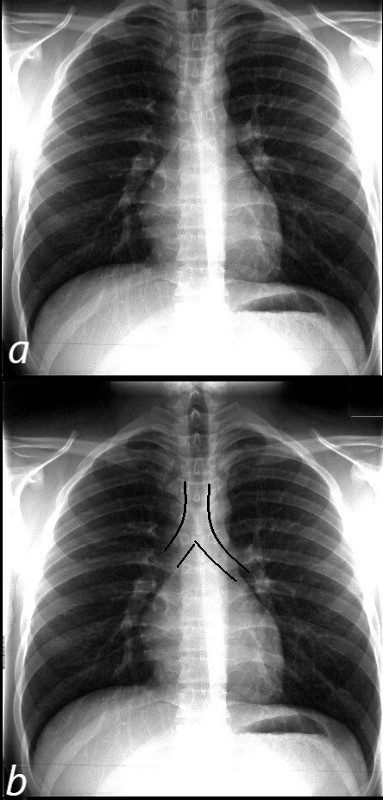
NORMAL FRONTAL CXR NORMAL ASYMMETRIC BRANCHING OF MAINSTEM BRONCHI
The normal CXR shows the characteristic asymmetric branching of the main stem bronchi. The right is short and stout and slightly more vertical while the left is long and thin and slightly more obtuse.
The normal carinal angle is between 40-80 degrees.
Ashley Davidoff MD
CARINAL ANGLE – 40-80 degrees
Ashley Davidoff MD
THE LEFT – TALL THIN AND GRACILE
The carinal angle

http://www.wikiradiography.net/
Courtesy Radiopaedia
 ET TUBE IN RIGHT MAIN STEM BRONCHUS
ET TUBE IN RIGHT MAIN STEM BRONCHUS
Anatomy of the Heart
Chambers that are Border Forming on the PA Examination
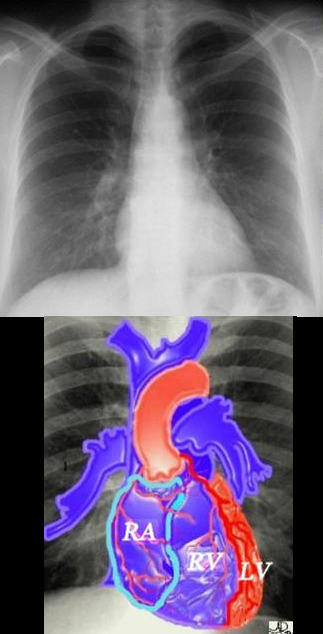
If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung. The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior view. It marks the position of the interventricular septum.
Ashley Davidoff MD
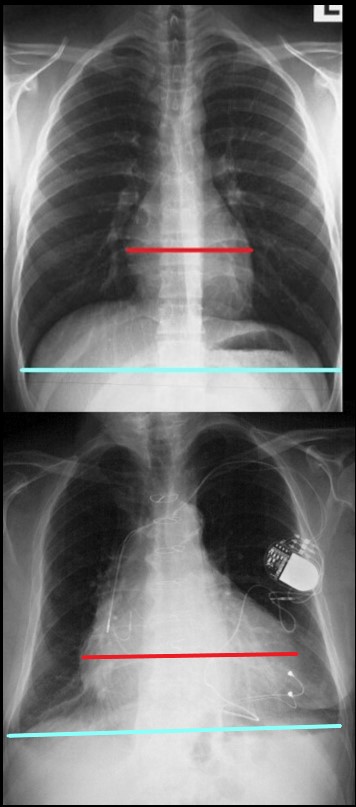
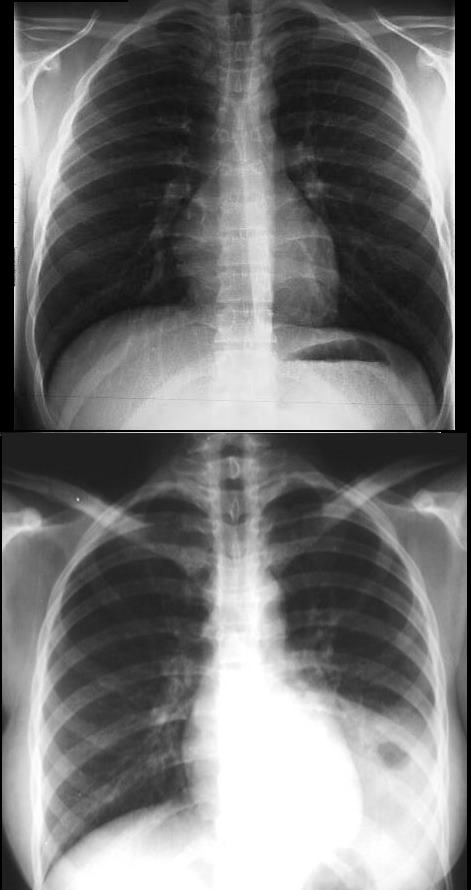
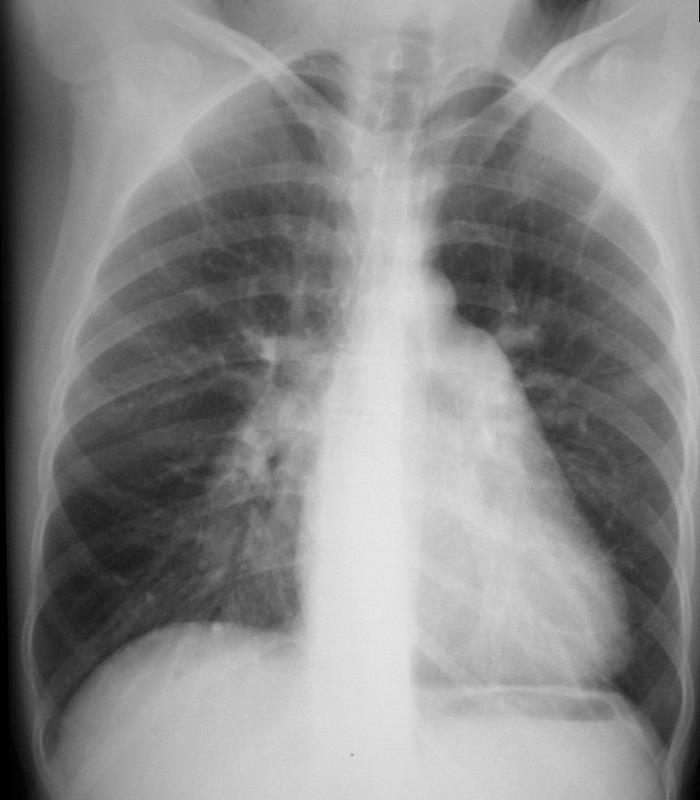
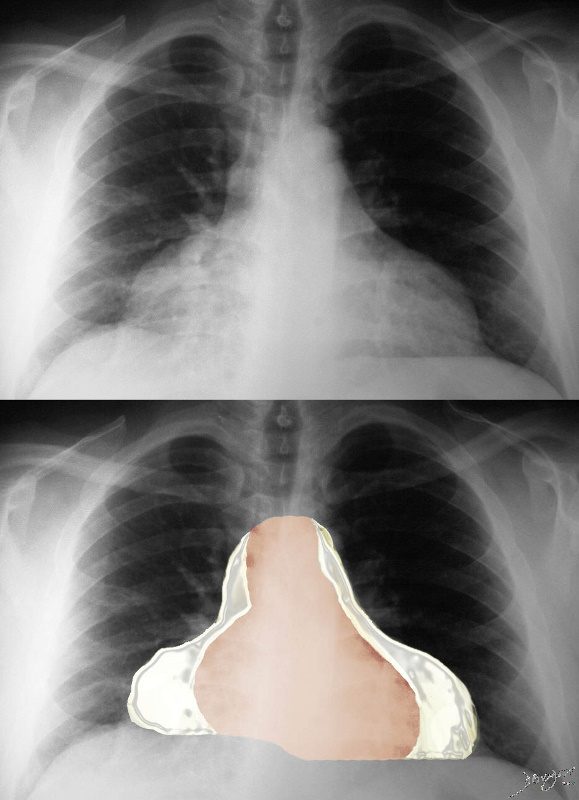
The maximum transverse length of the heart is expressed as a percentage of the maximum length of the internal diameter of the chest. When this ratio – the cardiothoracic ratio (c t r) is greater than 50% cardiomegaly is present. The top image is normal and the bottom reflects cardiomegaly
Ashley Davidoff MD
There are Two Basic Common Shapes of Cardiomegaly
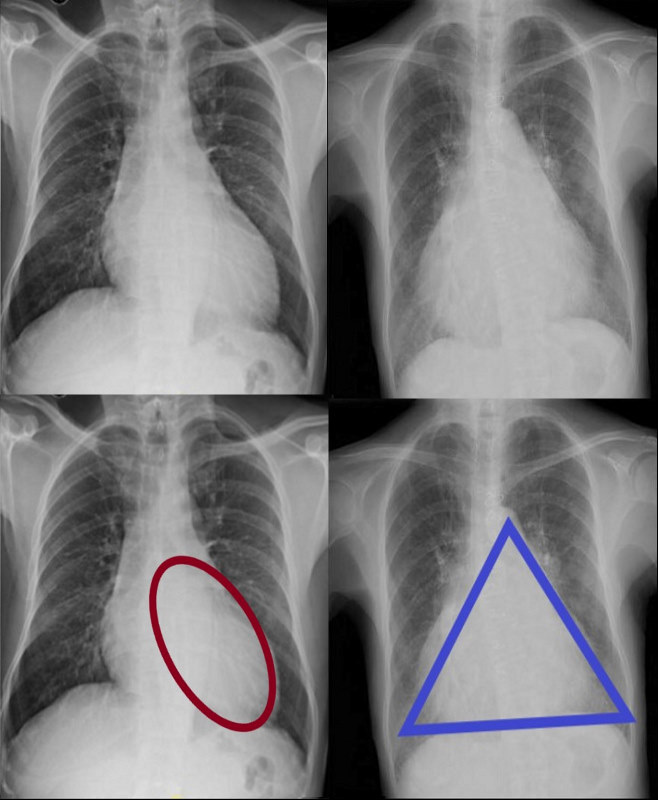
CARDIOMEGALY – TWO BASIC TYPES -OVOID and TRIANGULAR
The ovoid form which suggests left ventricular dominance and triangular form which suggests right ventricular dominance.
Ashley Davidoff MD
The Ovoid Form of Cardiomegaly – Consider LVE
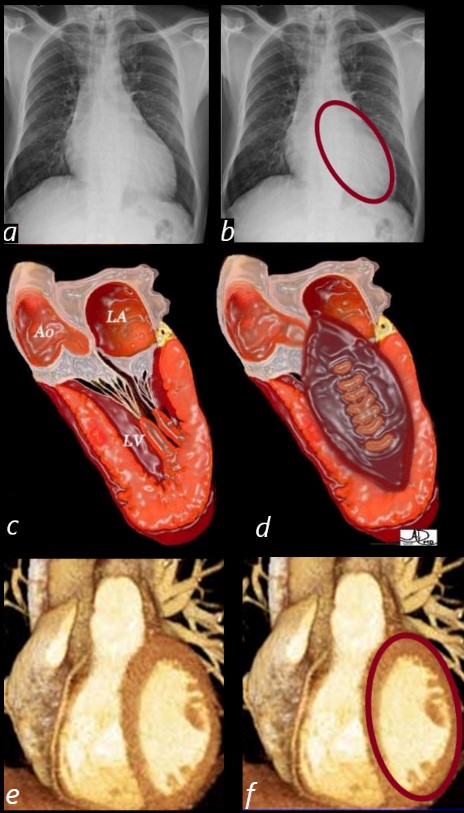
SHAPE OF THE LEFT VENTRICLE
The enlarged LV (a,b) is shaped like an oval and it is likened to a rugby ball or an American football placed on the field at kick off time. LVE on CXR is mostly assessed by an increased cardiothoracic ratio as well as the accentuation of the ovoid shape. (lower images c, d,e, f)
Ashley Davidoff MD
Vector of the Enlarging LV – Rotate Down and to the Left
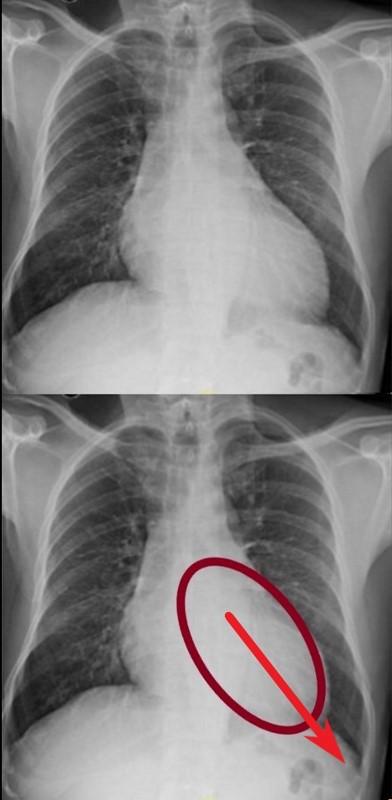 VECTOR FOR LV ENLARGEMENT
VECTOR FOR LV ENLARGEMENT
DOWN AND OUT
The left ventricle (LV) enlarges in a posterior, downward and lateral direction resulting in the characteristic changes of LVE on CXR
Ashley Davidoff MD
Clinical Exam – Focal LV Thrust
The left ventricle (LV) enlarges in a downward and lateral direction resulting in the apical impulse displacement and increase forcefulness of the apical tap.
Ashley Davidoff MD
62 year old female with acute chest pain atrial fibrillation, hypotension admitted to ICU. Clinical evaluation was considered to be non-ischemic cardiomyopathy with EF by echo of about 20%. She was hypotensive and, in the ICU, and CXR showed acute CHF with cardiomegaly. The TEE was more in keeping with segmental dyssynergy, Cardiac cath showed occluded RCA bot good collateralization from the LAD. MRI showed subendocardial LGE in the inferior and inferolateral portions of the LV consistent with a prior infarction and EF of 20%
Ashley Davidoff MD
The Triangular Form of Cardiomegaly
Consider RVE or any disease from the left side that may cause RVE eg mitral stenosis
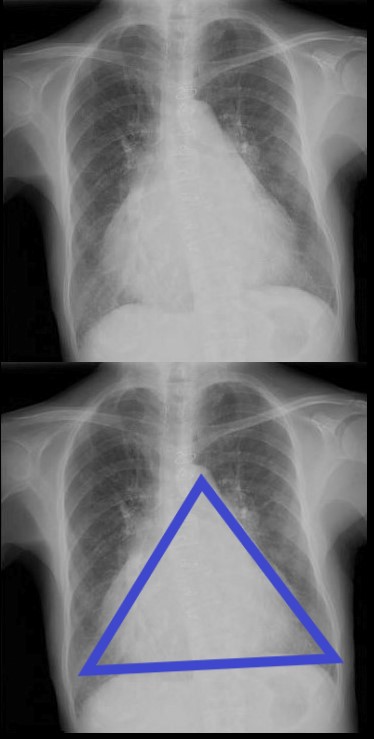
TRIANGULAR SHAPED HEART – SUGGESTING RIGHT VENTRICULAR DOMINANCE. MITRAL STENOSIS PULMONARY HYPERTENSION
71 year old Asian female with rheumatic heart disease dominated by calcific mitral stenosis mild MR, moderate tricuspid regurgitation and secondary pulmonary hypertension.
Ashley Davidoff MD
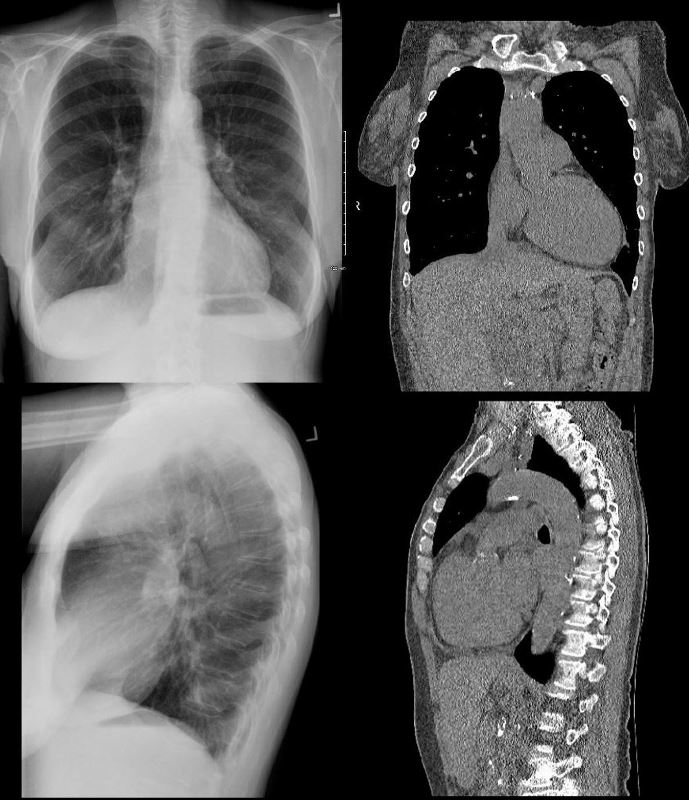
Note the Basic Shape of the RV is Triangular in almost all Views
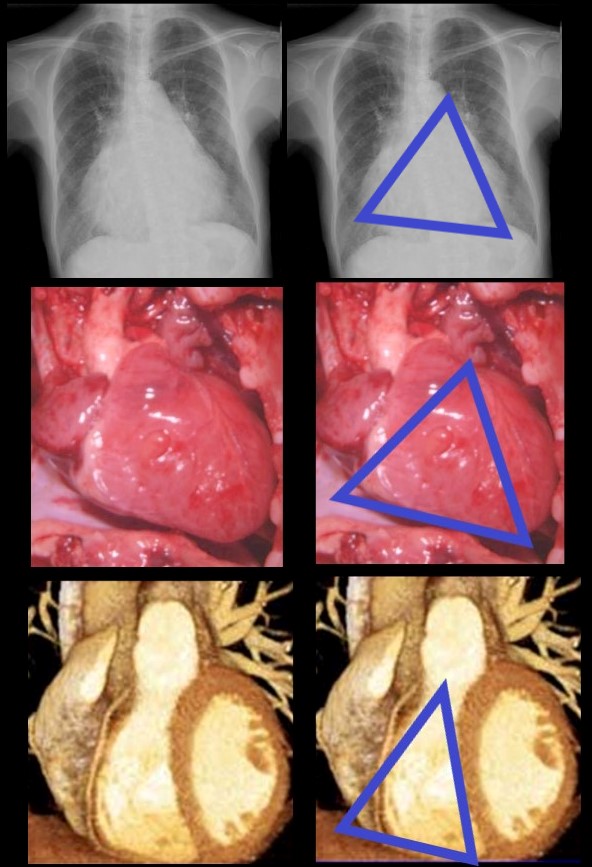
The enlarged LV (a,b) is shaped like an oval and it is likened to a rugby ball or an American football placed on the field at kick off time. LVE on CXR is mostly assessed by an increased cardiothoracic ratio as well as the accentuation of the ovoid shap. (lower images c, d,e, f)
Ashley Davidoff MD
Vector of the Enlarging RV – Rotate Laterally to the Right
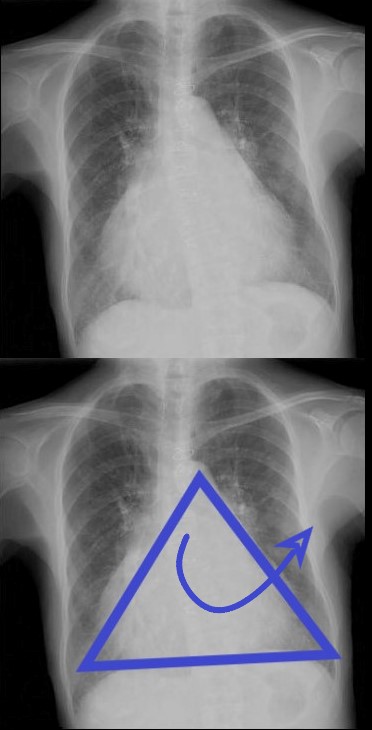
ANTERIOR LEFTWARD
The right ventricle (RV) enlarges with a clockwise rotation resulting in an upward turning of the apex and enlargement in a anterior and leftward lateral direction.
Ashley Davidoff MD
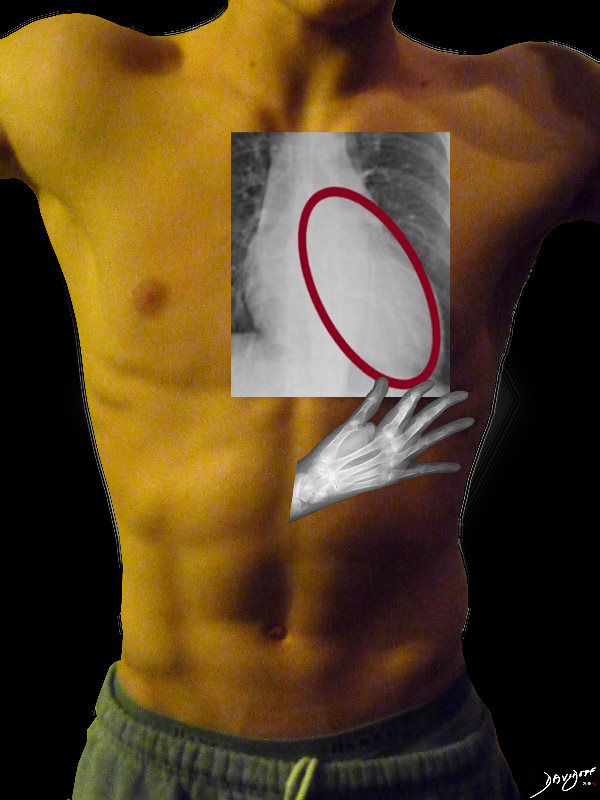
Clinical Exam of the RV – Diffuse Anterior Parasternal Heave
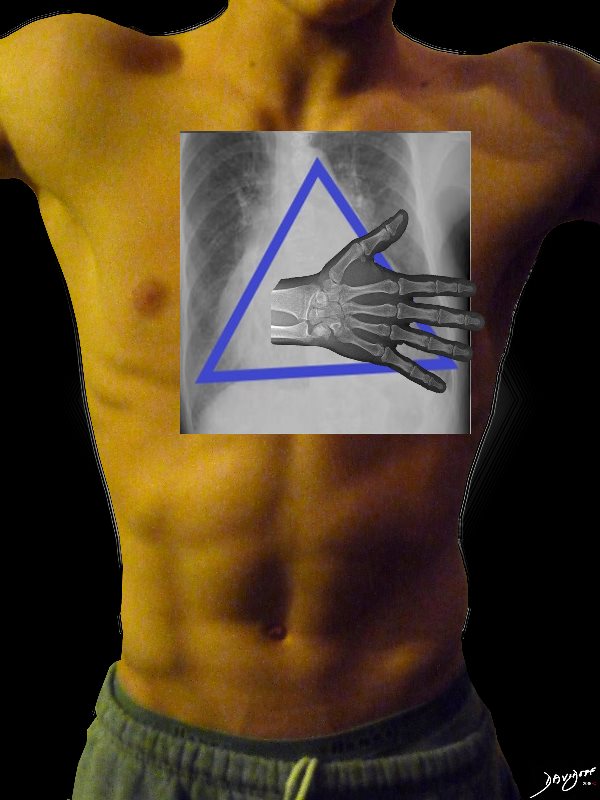
The right ventricle (RV) enlarges in a anterior, upward and lateral direction resulting in the broad based parasternal pulsation which on clinical examination is identified as a parasternal heave identified with the base of the extended hand
Ashley Davidoff MD
The Straight Left Heart Border

Triangular shaped heart with RVE LAE
Ashley Davidoff MD
The Main Pulmonary Artery
Normal
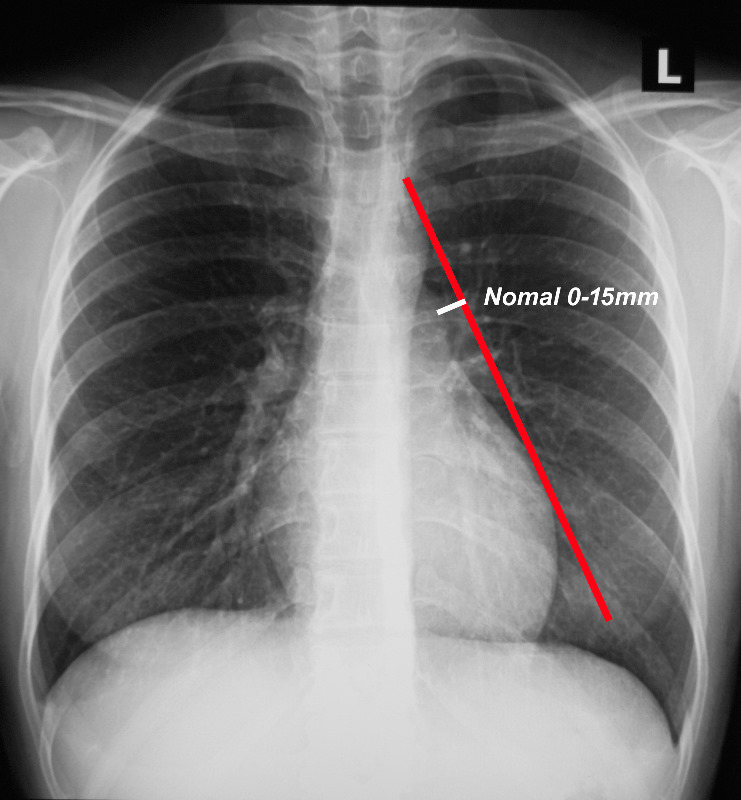
When a line is drawn from the aortic knob to the left edge of the heart, (red line) the pulmonary artery should lie medial to that line (ie along the line drawn to 1.5cms medial to the line)
Ashley Davidoff MD TheCommonVein.net
Pulmonary Hypertension
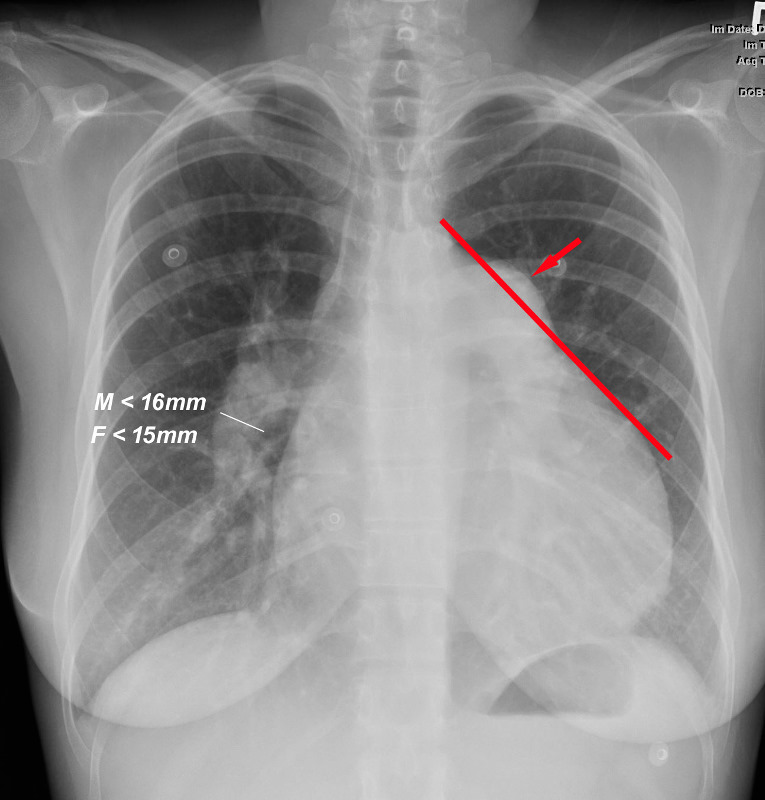
When a line is drawn from the aortic knob to the left edge of the heart, (red line) the pulmonary artery lies lateral to that line indicating an enlarged pulmonary artery most commonly caused by hypertension . In this instance the size of the descending right pulmonary artery is greater than 15 mms confirming the presence of pulmonary hypertension
Ashley Davidoff MD TheCommonVein.net
Frontal x-ray with triangular shaped heart due to pulmonary hypertension with enlarged MPA and enlarged descending RPA .
Ashley Davidoff MD
What about the Right Atrium (RA) and Right Heart Border?
The RA does not make much a statement on the frontal CXR unless very large
If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung. The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior view. It marks the position of the interventricular septum.
Ashley Davidoff MD
The Enlarged Right Atrium
The right atrium is the most difficult chamber to assess unless it is very large in which case it will manifest on the frontal CXR with a very large right paravertebral border.
-
- enlarged, globular heart
- narrow pedicle
- gross enlargement of the right atrial shadow, i.e. increased convexity in the lower half of the right cardiac border
- right atrial convexity is more than 50% of the cardiovascular height
- right atrial margin is more than 5.5 cm from the midline
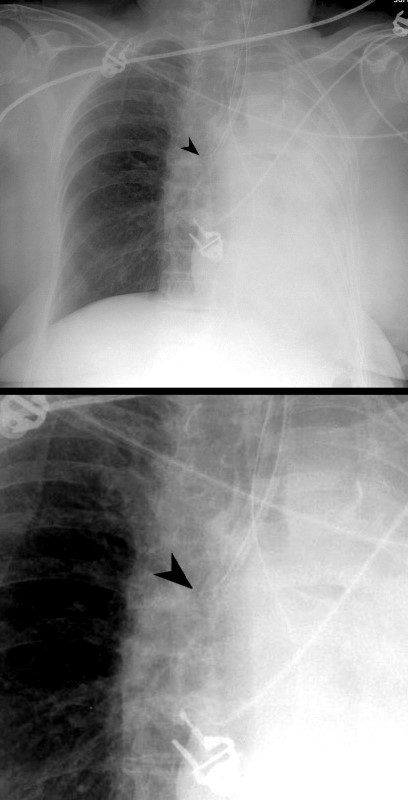
The right atrium is the most difficult chamber to assess unless it is very large in which case it will present on the frontal CXR with a very large right paravertebral border. This is a 71 year old female person with rheumatic heart disease with pulmonary hypertension and tricuspid regurgitation hence resulting in a large right atrium (RAE)
Ashley Davidoff MD
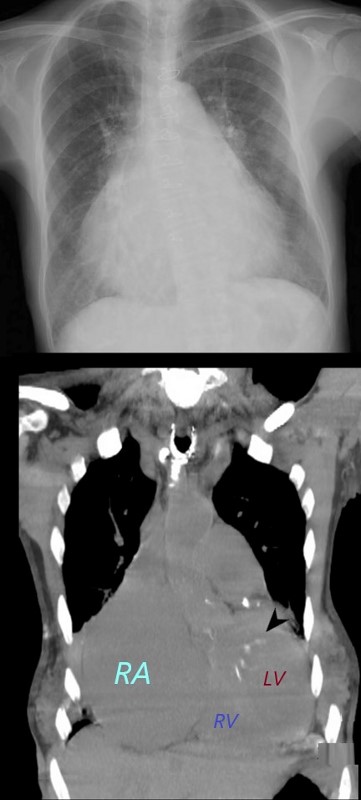
The right atrium is the most difficult chamber to assess unless it is very large in which case it will present on the frontal CXR with a very large right paravertebral border. The frontal CXR and coronal CT through the RA is from a 71 year old female with rheumatic heart disease with pulmonary hypertension and tricuspid regurgitation resulting in a giant right atrium (RAE). The RA accounts for the large bulge of the right border of the cardiac silhouette. The black arrowhead in the loer image points to the calcified mitral valve.
Ashley Davidoff MD
The Left Atrium
3 signs
-
- Carinal Angle
- Double Density
- Filling in of the Left Atrial Appendage Bay
The Carina and the Carinal Angle
NORMAL FRONTAL CXR NORMAL ASYMMETRIC BRANCHING OF MAINSTEM BRONCHI
The normal CXR shows the characteristic asymmetric branching of the main stem bronchi. The right is short and stout and slightly more vertical while the left is long and thin and slightly more obtuse.
The normal carinal angle is between 40-80 degrees.
Ashley Davidoff MD
ASYMMETRIC BRANCHING PATTERN – RIGHT SHORT AND STOUT AND THE LEFT LONG AND THIN
CARINAL ANGLE – 40-80 degrees
Ashley Davidoff MD
The Abnormal Carinal Angle

A dancer demonstrates a normal carinal angle (upper image) and as she continues to extend her left leg, (lower images) the angle becomes greater than 80 degrees and in terms of the carinal angle becomes abnormal.
Ashley Davidoff MD
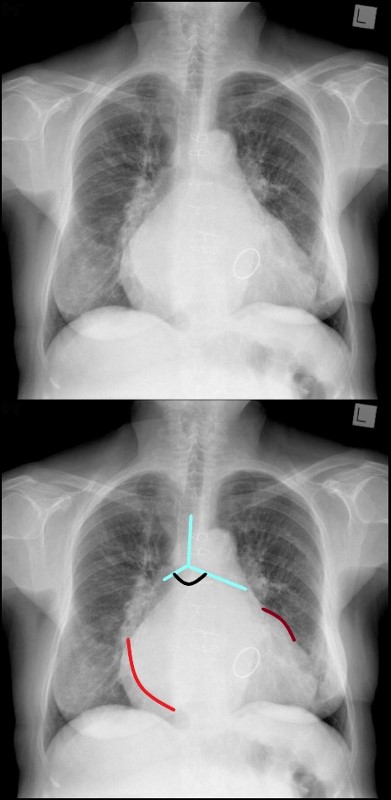
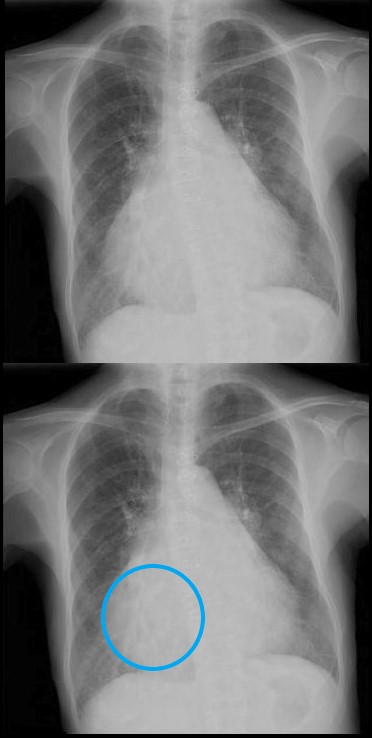
MITRAL STENOSIS WITH ENLARGED LEFT ATRIUM – WIDENED CARINAL ANGLE DOUBLE DENSITY ENLARGED LEFT ATRIAL APPENDAGE
The frontal CXR demonstrates findings consistent with mitral stenosis including a widened carinal angle (teal blue and black arc), a double density (red arc) and an enlarged left atrial appendage (maroon arc).
The overall shape of the heart is triangular suggesting right ventricular enlargement. A mitral valve prosthesis is in position
Courtesy of Radiopaedia
-
-
-
Where to Look The Physics of Air and Fluid
-
Gravity, Air and Fluid
-
-
Gravity Air and Fluid
Remember the roles they play in Supine and upright projections
Ashley Davidoff thecommonvein.net -
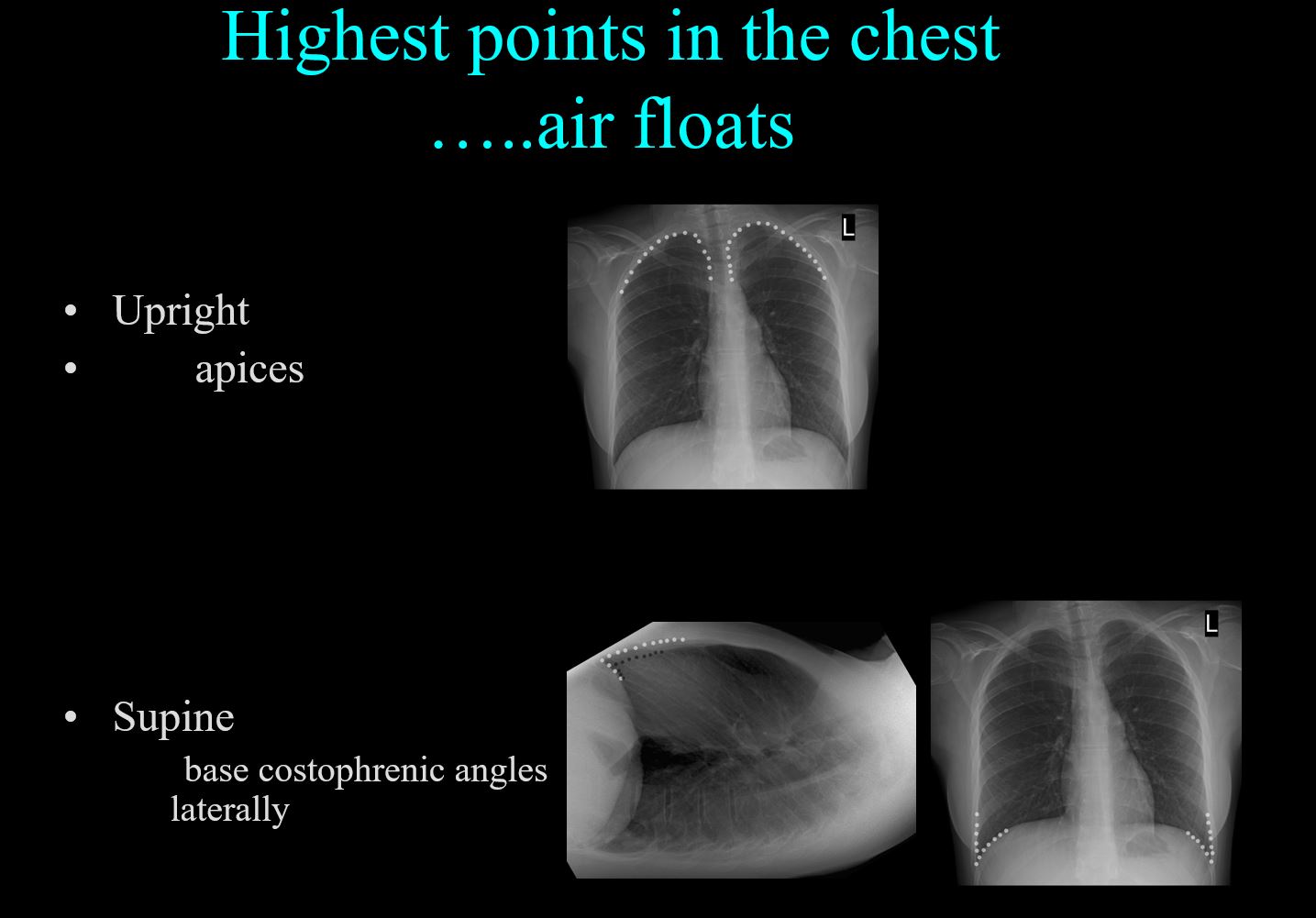
Air in the Upright and Supine Projection
Ashley Davidoff thecommonvein.net
-
- Pneumothorax
-
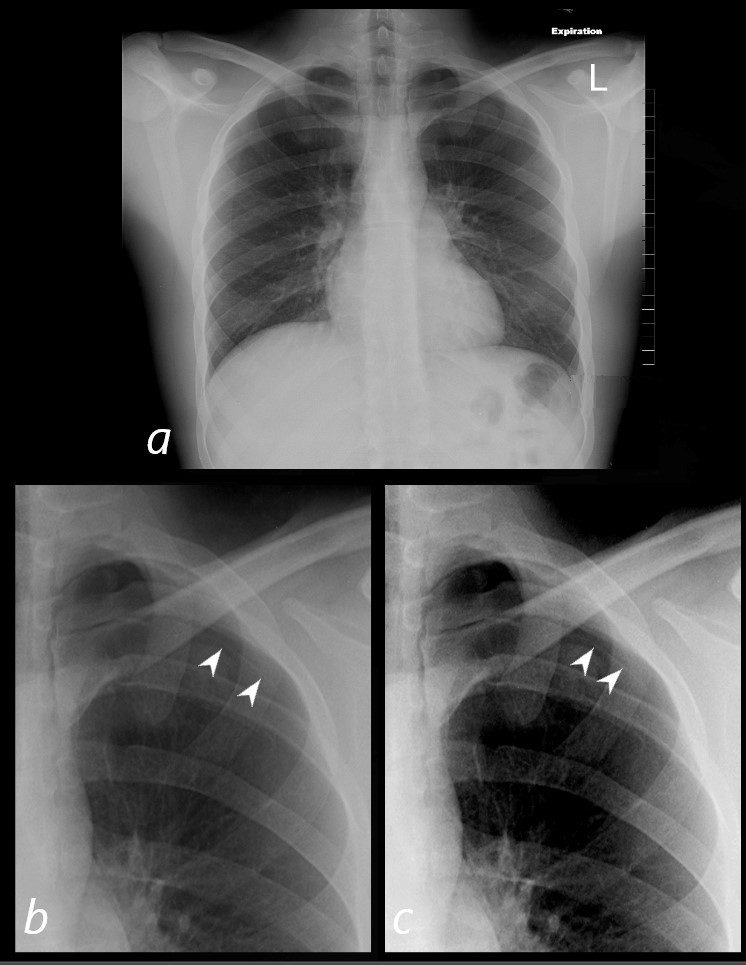
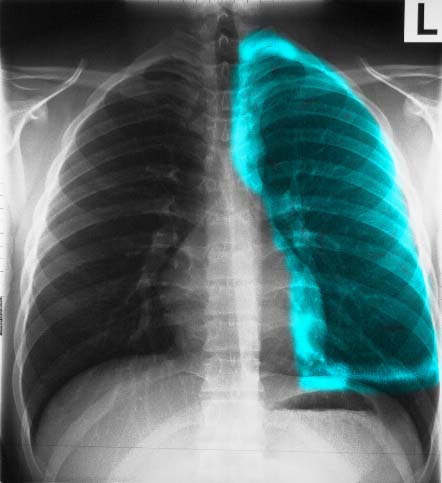
SMALL APICAL PNEUMOTHORAX IN AN UPRIGHT CXR TAKEN IN EXPIRATION.
In an upright position a pneumothorax rises to the apex of the lung and assumes the shape of the apex because it exerts pressure on the lung apex which yield to the greater pressure. The expiration film accentuates the pneumothorax because it further reduces the pressure in the lungs and increases the pressure difference between the PTX and the intraparenchymal pressure.
The PTX is barely seen in (a) and is better seen in the magnified views (b and c) and with increasing contrast (c) the faint line of the the pleura becomes better visualized (white arrowheads).
Ashley Davidoff MD -
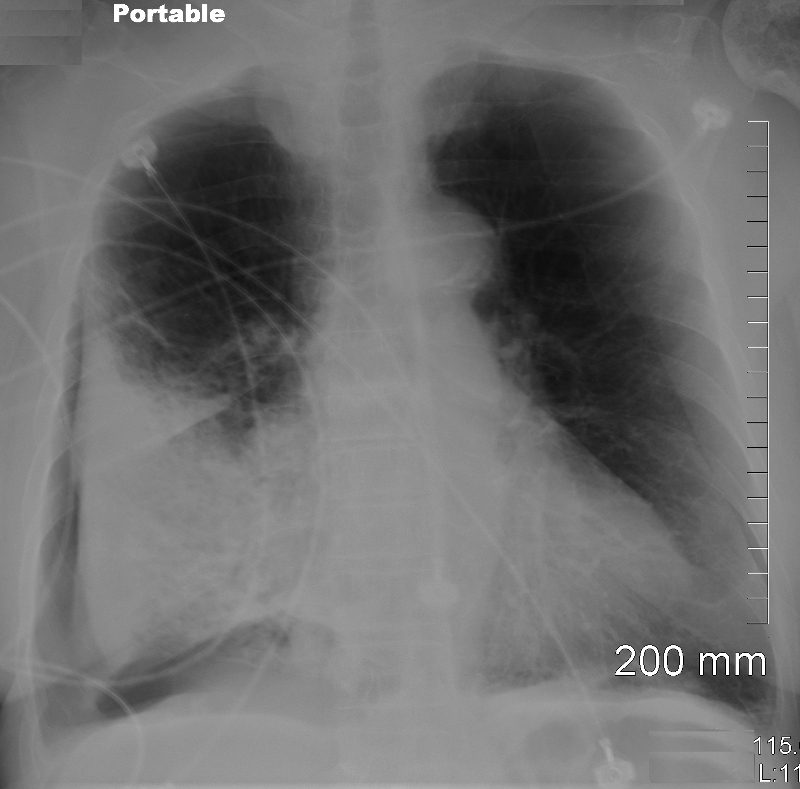
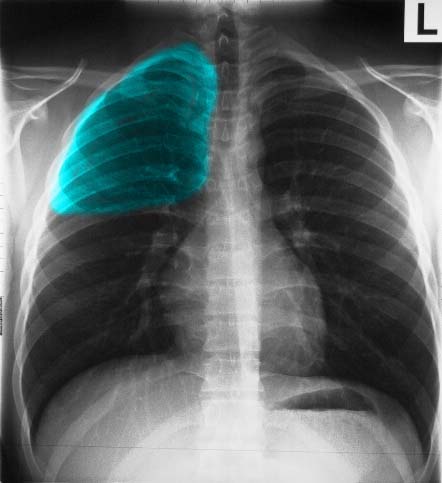
DEEP SULCUS SIGN
Portable supine examination in the ICU shows a pneumothorax in the right subpulmonic region
Ashley Davidoff MD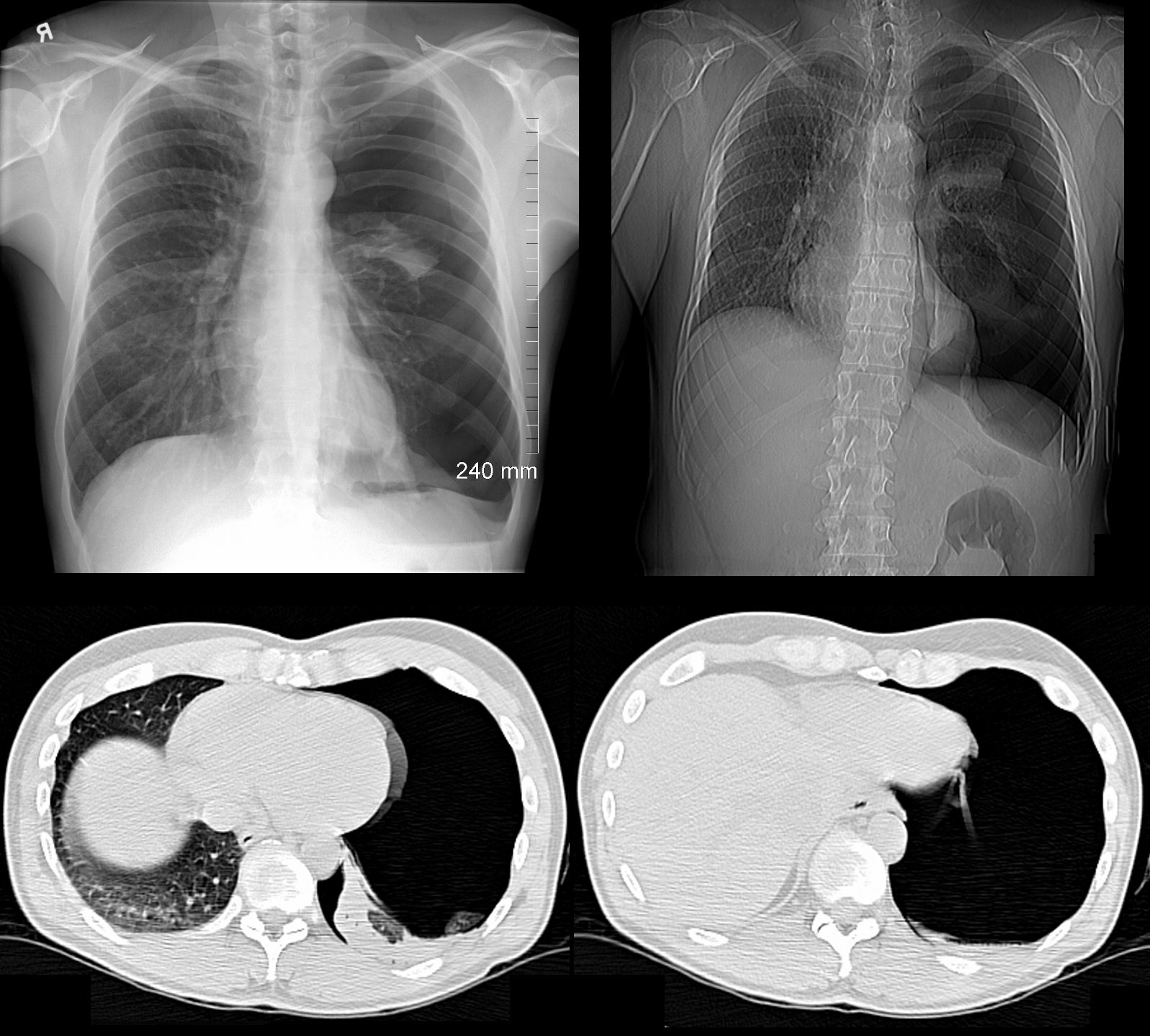
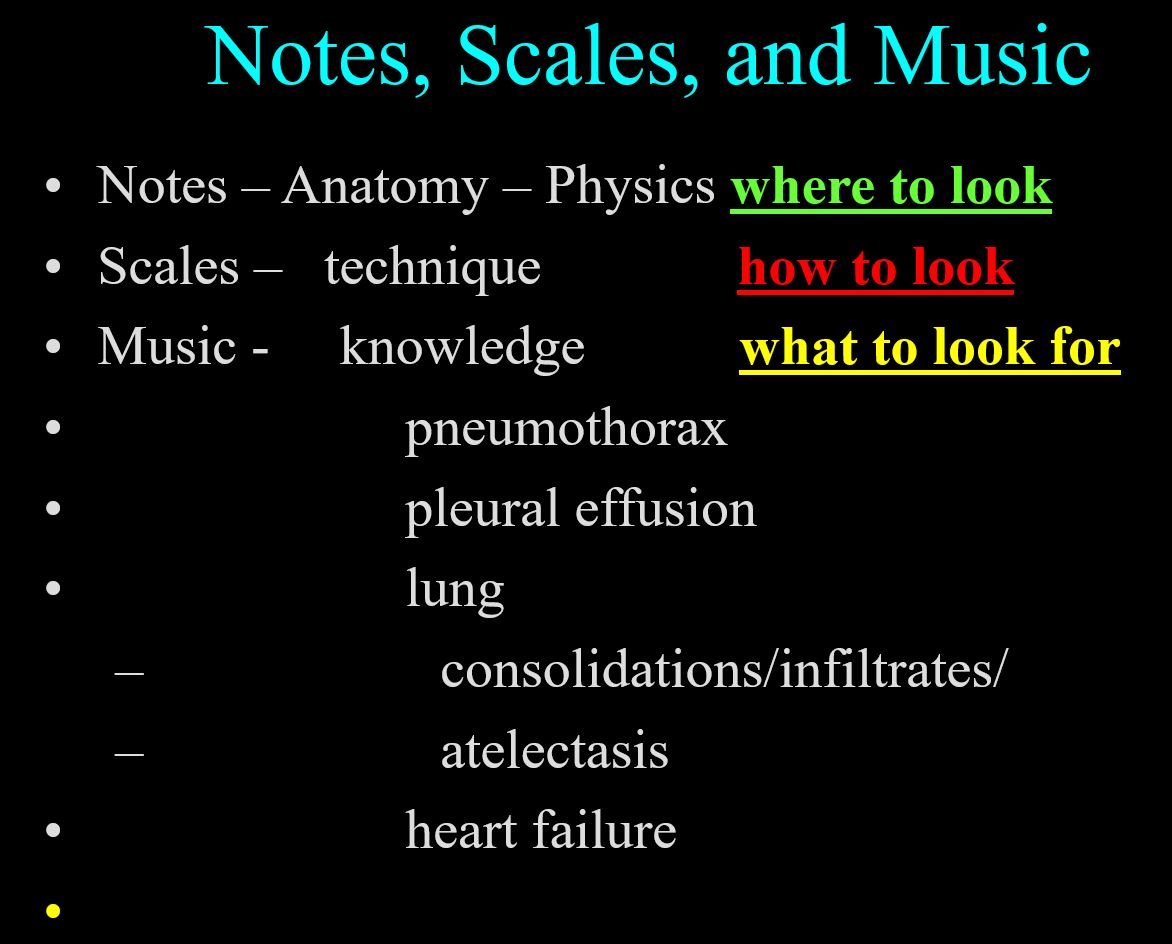
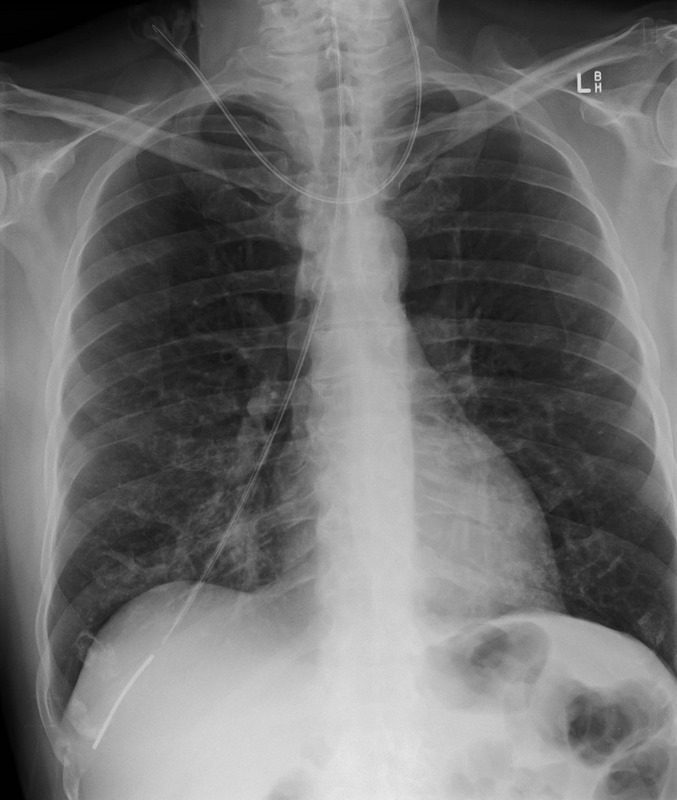
Spontaneous Tension Pneumothorax
49 year old male with a cough presents for a Chest Xray which showed a tension pneumothorax. Chest tube was placed emergently in the radiology department.
Ashley Davidoff MD TheCommonVein.net
117300cPleural Effusion
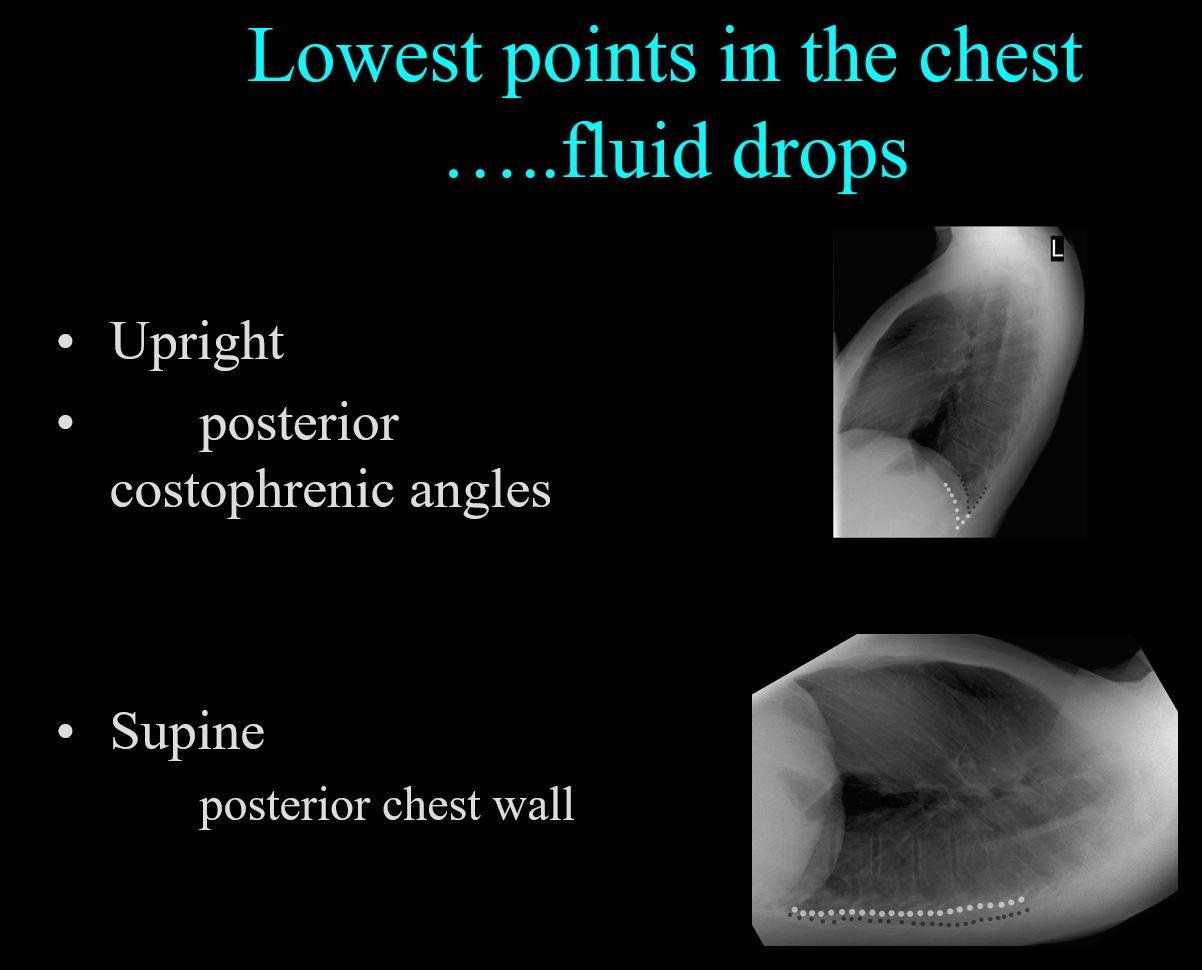
Fluid in the Upright and Supine Projection
Ashley Davidoff thecommonvein.net -
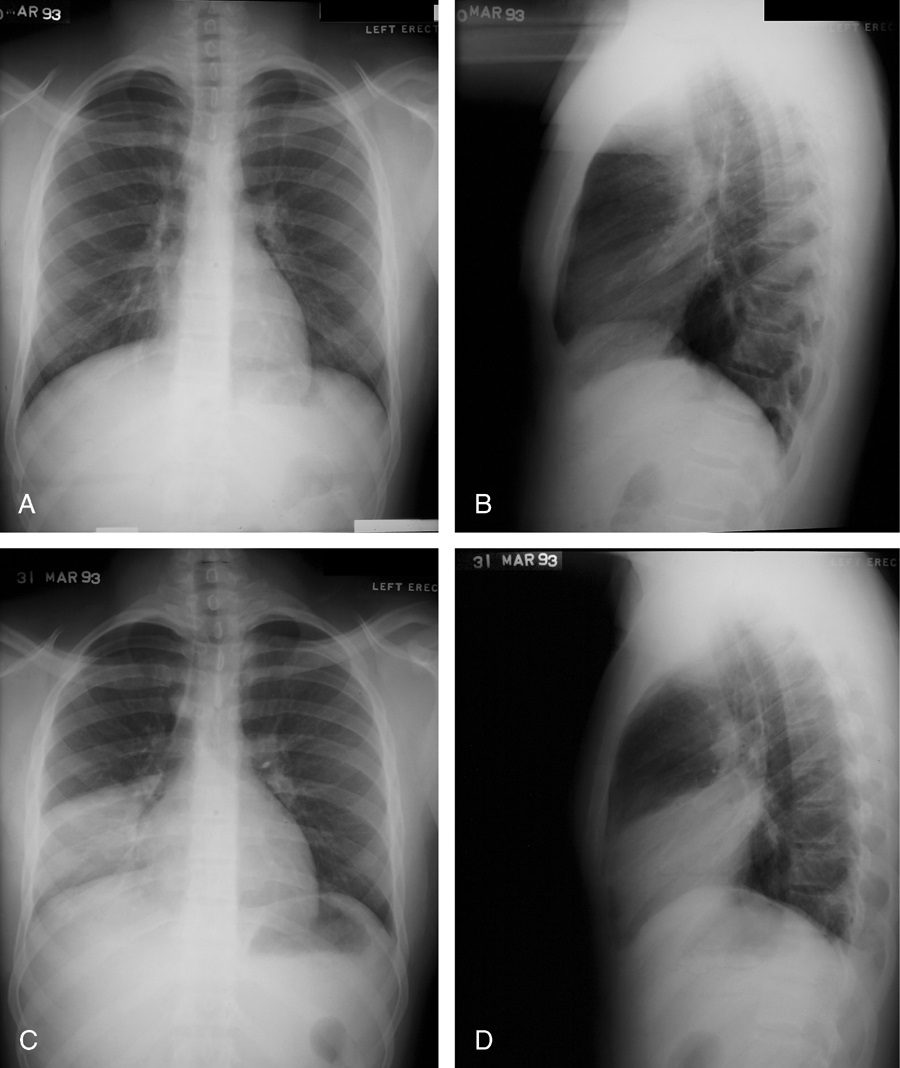
Small Effusion May Only Seen on the Lateral Exam
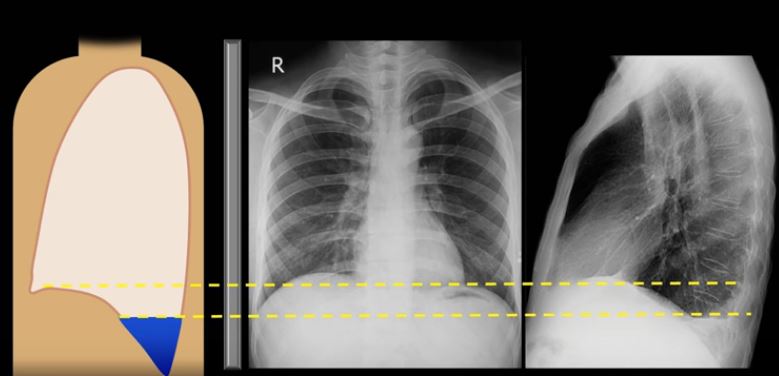
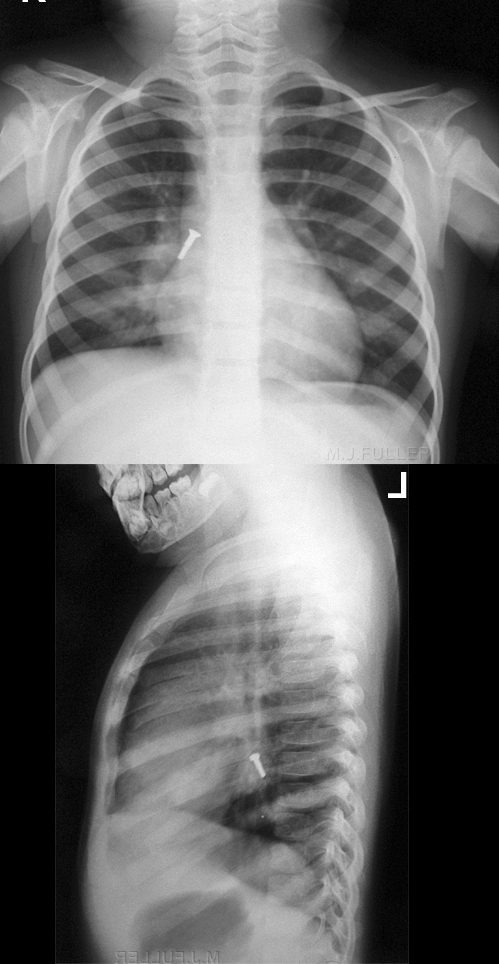
SMALL EFFUSION ONLY IDENTIFIED ON THE LATERAL EXAMINATION
A small effusion is not identified on the PA chest since it is hidden by the diaphragm and the effusion first fills the posterior recess because it is most inferior. The lateral examination is required to identify the effusion
Courtesy How to Interpret CXR Strong Medicine
https://www.youtube.com/watch?v=wOpDvUO5sD8 -
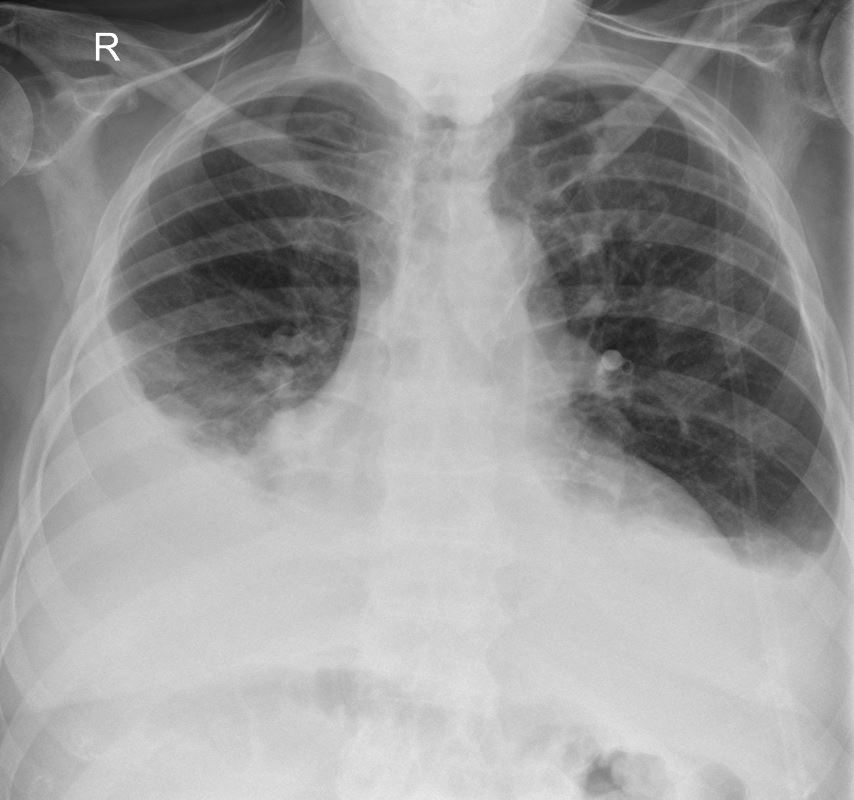
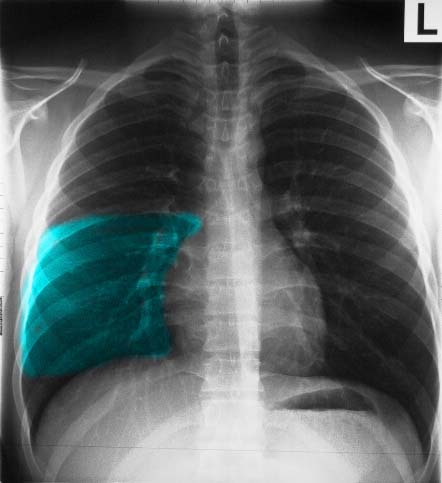
Typical shape of a moderately large right pleural effusion
Case courtesy of RMH Core Conditions, Radiopaedia.org, rID: 34401 -
Veiling Opacity
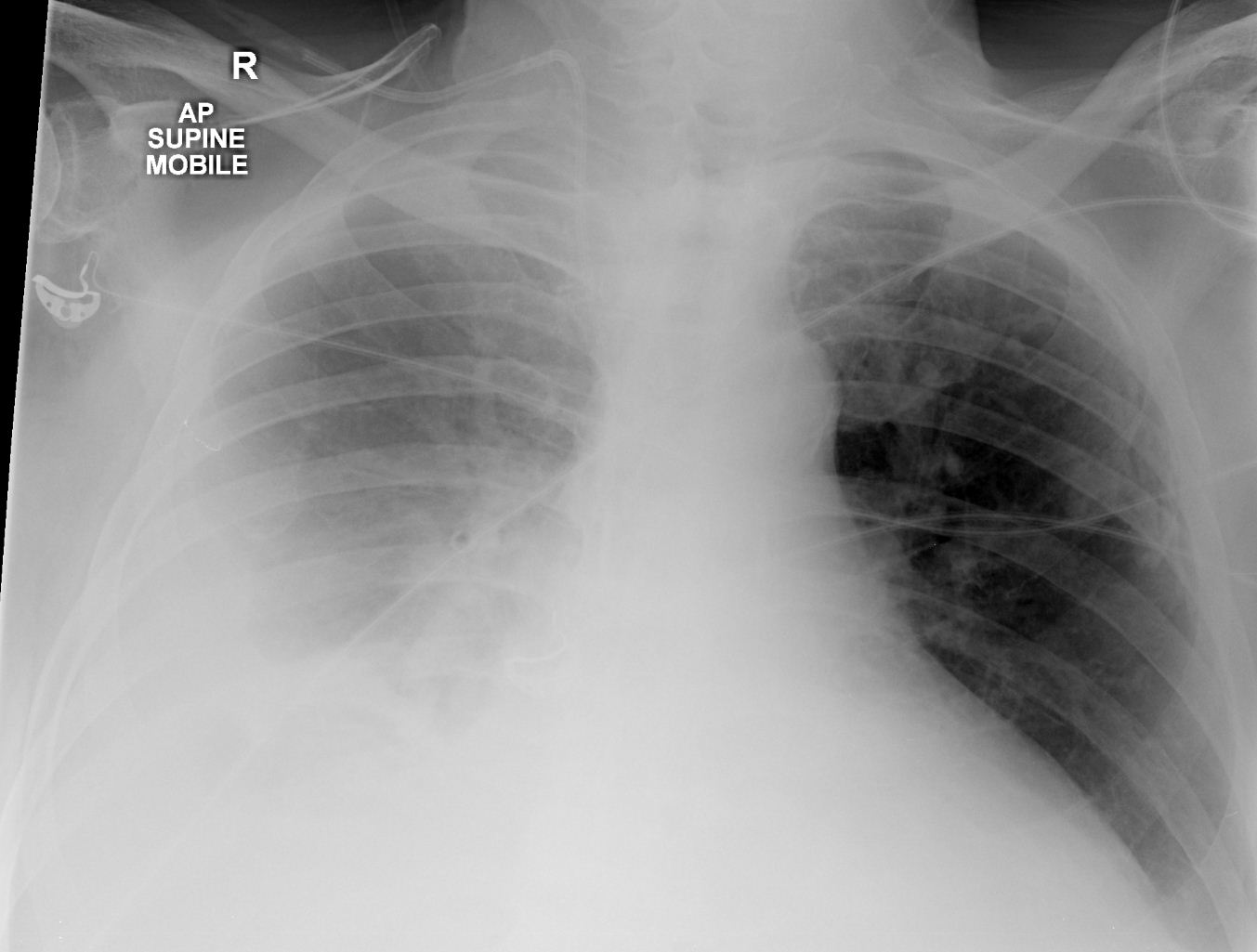
Veiling Opacity left pleural effusion in the supine projection
Case courtesy of RMH Core Conditions, Radiopaedia.org, rID: 34401 -
Scales
-
Learning how to look so that you can see
-
How to look and
what to look for
Ashley Davidoff thecommonvein.net -
Notes Scales and Music
- Scales
- Have a fluid and logical method of looking (search pattern) and
- practice practice practice
- Have a fluid and logical method of looking (search pattern) and
-
SCALES
- 4 Review Spaces relating to 4 areas of major disease
- Pleura – PTX and Effusions
- Lungs – Pneumonia and Masses
- Hila – Masses and CHF
- Heart – Megalies and Failure
First Scale – Pleural Run

Ashley Davidoff MD
Pattern – start at the white lines to the right and left of the thoracic vertebra running along the diaphragms into the pleural recesses, up the lateral walls to the apices
2nd Scale – Lung Loops

Ashley Davidoff MD
- Pattern –
-
- Come down the trachea and and
- loop the upper lung fields, then the
- mid lung fields, and finally the
- lower lung fields
- looking for
- symmetry,
- masses,
- infiltrates,
- interstitial changes
-
3rd Scale – Skiing on the Moguls

A methodical approach to evaluation of the cardiac silhouette is likened to skiing down a mogul laden ski slope and then taking a trip on the ski lift back to the top of the mountain. The ski slope starts at the left subclavian artery (light brown)
, followed by the mogul of the aortic knob (bright green) at the bottom of which is the A-P window (white) only to be presented with a second mogul of the main pulmonary artery(yellow), and then the bay of the left atrial appendage (pink)and finally free at last of moguls and an exciting and accelerating ski down the LV (red)
We then have to take a walk back to the ski lift. At the junction of the LV (red) and the RV (blue) , if we take a right ward look up the mountain we can spot the LAD on top of the interventricular septum.
The walk along the border of the RV is terminated at the junction of the RV (dark blue) and the right atrium (light blue). At this point we wait in line to get on to the ski lift. We ride up the right hand border of the right atrium (light blue) a little rough bump over the ascending aorta )maroon) and then straight to the top along the SVC (pink).
Ashley Davidoff MD
- Pattern of the Ski Run –
- Start at the left apex at the left subclavian artery,
- jump the aortic mogul and
- land in the AP window, and then
- jump the PA mogul,
- land in the LA appendiceal bay, and then
- ski all the way down the LV.
- Walk back to the ski lift via the inferior border of the RV and then the RA.
- At the bottom of the RA get on to the ski lift as the IVC enters the RA
- and then take the lift up the mountain via the RA ,
- portion of the ascending aorta and the
- the SVC
4th Scale – Hilar Hoops
- Pattern of the Hilar Hoops –
-
- Trip down the trachea – Specifically to look at the carinal angle
- Upper hoop specifically to look at pa- bronchus ratio
- Middle Hoop – Specifically to look at hilar size and shape
- Lower Hoop – Specifically to look for redistribution and clarity of RPA
-
-
-
-
-
Pericardial Effusion
WATER BOTTLE HEART
X-ray shows the typical appearance of a “water bottle heart” characteristic of a pericardial of a large pericardial effusion.
Ashley Davidoff MDsn chest integrated 09ep finding br3 imaging
Word First Definition air bronchogram atelectasis bleb <1-2cms bronchiectasis bulla >1-2cms congestive heart failure (CHF) consolidation effusion pleural (small, large, subpulmonic, decubitus films, supine and upright) ground glass opacity (GGO) mass solid lung mass >3cms nodule solitary pulmonary (spn) <3cms pneumothorax (small, large, supine and upright, decubitus and expiratory films, tension) pneumothorax tension silhouette sign white out opacification distinguishing causes of hemithorax (effusion, vs vs pneumonia vs pneumonectomy)
-
-
-