copyright 2009
Introduction
Size is one of the most important universal descriptors of structure. It is a measurable entity, and determining whether a structure is normal or abnormal can be verified against a normal standard. The red cell is about 5-7 microns in diameter, and the normal liver weighs 1400grams, for example. Size and weight of many organs differ between the sexes and among age groups. Measurements may be linear, portray a volume, mass, rate or frequency. Size may be reflected as a ratio, such as the very important nuclear/cytoplasmic ratio of the cell. The relevant concept is that it is important to group these facets under the umbrella of “size” and to understand that all descriptors relating to magnitude can be viewed as being a descriptor of size, whether in grams, cms/sec, or nuclear cytoplasmic ratio. By grouping all these quantifications under the concept of “size”, a framework is provided for the detail, which will enhance understanding. (or “standing under” the detail). ** This is the “lumpers”, rather than the “splitters” approach described and referenced to McKusick in chapter 1.
Learning about structure requires an understanding and knowledge of the normal size. In the clinical realm, the size of examinable organs eg the heart liver or spleen is an essential consideration in the the evaluation of its health.
|
Normal and Morbid Obesity |
|
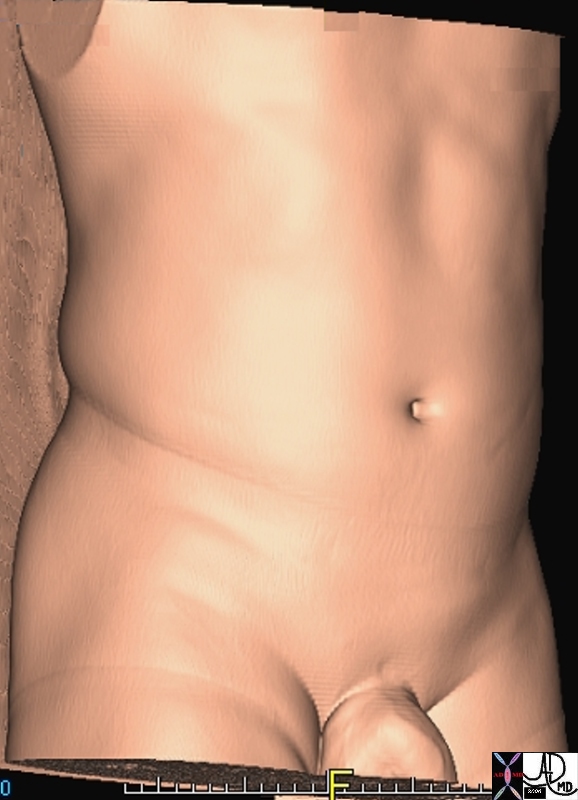
These images are derived from reconstructed CT images from a normal (left) and an obese patient (right). The manner in which the excessive tissue lays in folds in the obese patient, reflects that the excess tissue is due to the deposition of fat in the subcutaneous layers. Shape is a clue to the cause of the enlargement. 49609c02 abdomen health disease normal obese morbid obesity order disorder Davidoff MD |
|
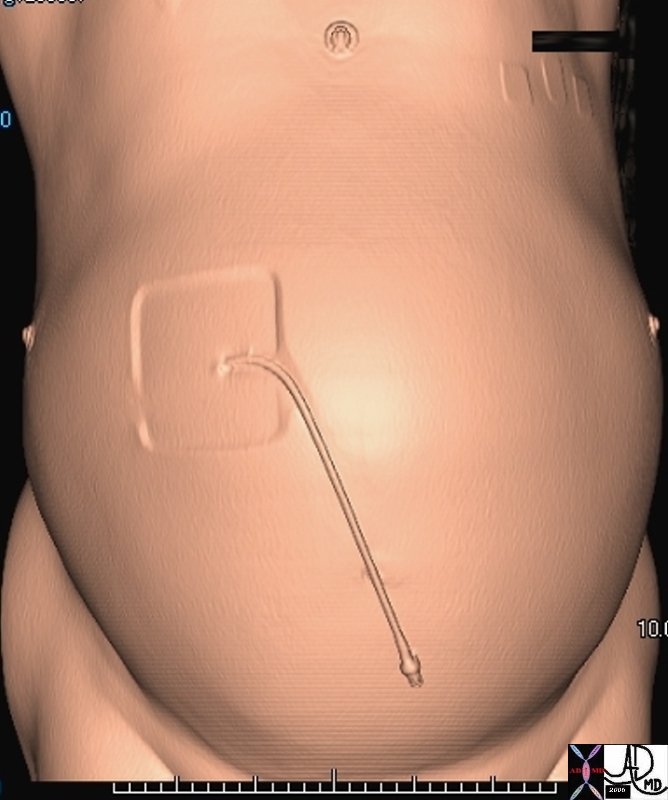
The Big Abdomen Normal (left) and Enlarged Abdomen (right) |
|
In this instance the size of the abdomen is abnormally large, but the shape, another descriptor of structure is abnormal as well. The rotund shape suggests increased tension in the abdomen and is characteristic of a condition called ascites marked by the accumulation of fluid in the peritoneal cavity. The catheter seen on the outside is used to remove the fluid intermittently and relieve the tension in the abdomen. 45883.800 46133b03 abdomen skin size fx enlarged distended shape CTscan Cortesy Ashley Davidoff MD |
|
The Enlarged Organ Normal (left) and Enlarged Spleen (right) |
|
The axial CTscans are from two different patients. The spleen in a, and overlaid in b is normal. The spleen in c and overlaid in d is enlarged. An extensive list for the differential diagnosis for splenomegaly exists and in large part the potential diagnosis is narrowed based on the background setting of the patient and associated clinical and imaging findings. 20712c01.8s CTscan spleen normal enlarged splenomegaly |

|
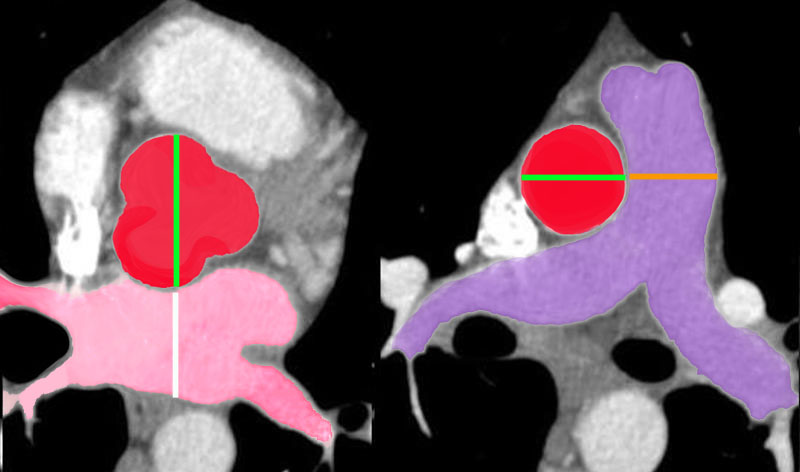
Normal and Enlarged Heart |
|
Two patients showing the normal cardiac silhouette on the left image and an enlarged triangular shaped heart on the right. One of the structures that is enlarged in this instance is the left atrium. In the second pair of images the normal left atrium is outlined in red. In the third set of images the enlarged left atrium is outlined in red as well. In this instance the left ventricle is normal in size and the right ventricle is enlarged characterized by the upturned apex of the heart. Mitral stenosis is the most likely diagnosis based on the enlargement of the left atrium and right ventricle. Courtesy of Ashley Davidoff M.D. 32113 code cardiac heart normal disease LAE RVE imaging radiology CXR plain film |
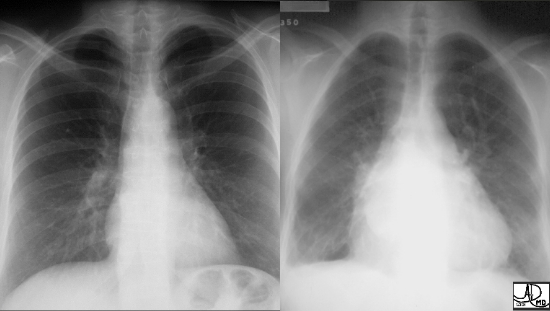
When a structure enlarges in disease,, the cause of the enlargement can be approached in many ways. An anatomical differential diagnosis is one place to start. First, the parts of the structure being analyzed must be identified. Next, the enlargement should be localized to one or more of these components. If a heart is enlarged on a chest X-ray an important branch point depends on determining whether the left side is abnormally big, the right side or both. Left sided enlargement allows deduction that the left atrium and or left ventricle are enlarged. If it is finally established that the left ventricle is normal and the left atrium is enlarged, then stenosis of the mitral valve becomes the most likely candidate for the cause of the disease. Since mitral stenosis in an adult is almost always caused by rheumatic fever, one can further deduce that the cause of mitral stenosis was a pediatric infection with Lancefield type A beta hemolytic streptococcus bacteria. The patient probably acquired cardiac involvement from streptococcus pharyngitis when he or she was between 5-15 years. The polymers in the wall of the organism, called M proteins, are highly antigenic and at the time forced the patient’s defense mechanism to create antibodies. While responding to the foreign organism, these antibodies also inadvertently react to the patients own tissues, including the myocardium, and or mitral valve, and possibly the pericardium, brain and even joints. The depth of the detail in the diagnosis depends on the doctor’s knowledge, but the story would not have been a story, and the diagnosis would not have been made, and treatment would not have been instituted, had a diagnostic finding not been identified – in this case the change in size of the heart. The beginning of diagnosis, even if it involves complex disease, starts with simple observations of aberrant structure or function. In this case it started with the simple observation of a change in size.
|
The Big Artery Normal (a) and Abdominal Aortic Aneurysm (b) |
|
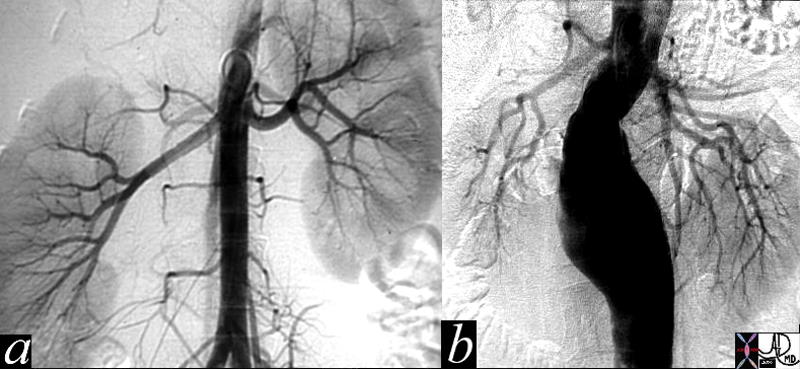
In the angiograms shown above the normal abdominal aorta (a) is shown in contrast to the aneurysm in b. As the radius of a structure increases, the tension on the wall increases. At a certain dimension, this tension can cause life threatening rupture. In the abdominal aorta the indication for elective surgery is 5.5cms. 11976c01 aorta abdomen abdominal aorta renal afrteries kidney fx normal AAA abdominal aortic aneurysm horseshoe kidney angogram angiography lumbar arteries Davidoff MD |
The importance of size cannot be overstated. Abnormal size can even be a predictor of life threatening events. The size of an aneurysm, an outpouching of a vessel, is an important indicator for its potential to rupture. Abdominal aortic aneurysms are relatively common in the aging population, due to inevitable loss of elasticity and weakening of the wall by atherosclerotic change. These changes result in ectasia or widening of the aorta. When the diameter of a segment of the aorta is 1.5 times wider than the normal segment of aorta above it, then it is classified as an aneurysm. When an infrarenal abdominal aortic aneurysm reaches a diameter of 5.5cms (normal about 2.5cms.) surgical repair is indicated because studies have shown that the risk of rupture starts to increase significantly when size advances beyond this point.
The importance and relevance of size continues as we examine structures under the microscope.
|
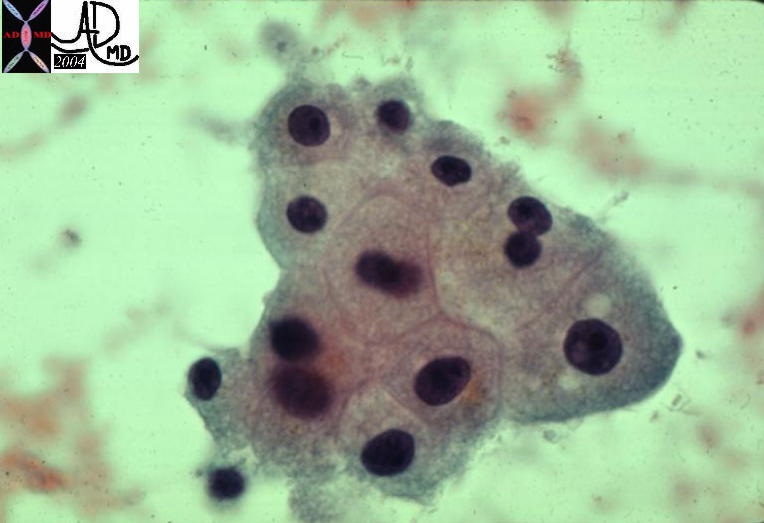
Nuclear-Cytoplasmic Ratio The normal (left) and the abnormally large nucleus (right) |
|
Two histological sections above show a normal nuclear cytoplasmic ratio of some liver cells on the left and cells with an increased nuclear cytoplasmic ratio on the right indicating malignant change. The experienced eye and mind of the pathologist develops a geshtalt of what the normal ratio. This is a difficult measurement to make objectively. 13440 13447Courtesy Barbara Banner MD
|
In this instance, making the assessment of an increase in the nuclear to cytoplasmic ratio is of the highest importance in the patient’s prognosis. If the nuclear cytoplasmic ratio is increased then a major criterion in the diagnosis of malignancy is recorded by the pathologist. The distinction between making a diagnosis of life threatening malignancy or not is as simple yet profound as that. It has its basis in the assessment of size.
Many diseases result in structures getting bigger. These encompass a variety of structural changes including neoplasia, hyperplasia, and hypertrophy. Diseases may also be caused by smallness of structure, with examples such as atrophy, hypoplasia, aplasia and atresia. Other disorders that may be associated with smallness include infarctions of the brain or spleen, congenital disorders such as hypoplastic right heart syndrome and esophageal atresia (esophagus is small and not formed) and immune disorders where tissue is destroyed such as sprue, or atrophic gastritis.
Evaluation of the magnitude of structure (and function in many ways) is a fundamental aspect of medicine. It is difficult to have a sense of how size fits into the clinical picture when it is learned in the context of basic science, but it always holds tremendous importance in the clinical realm.
The evaluation of size can take many forms. Most the time in medical imaging we consider a linear measurement since it is the easiest for us to measure. Yet other dimensions including mass, weight, velocity, volume, frequency, velocity, and concentration, are in some way a reflection of size as well
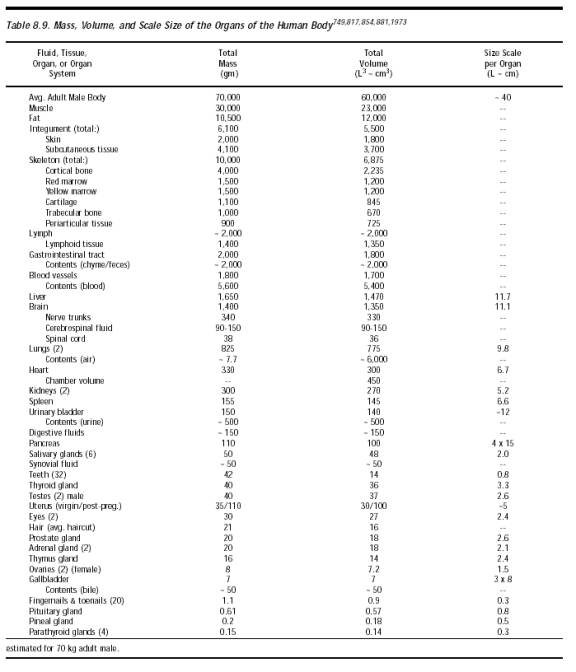
It may be useful to review the size of some common structures both at an anatomic level as well as a microscopic level in order to get a perspective.
The largest organ in the body is the skin, and the largest gland in the body is liver. The liver weighs about 1200 grams. Other large organs include the lungs which by volume are the largest, but by weight are not. The femur is the largest and longest bone in the body. The intermediate size organs include the brain heart, spleen and kidneys. The smaller organs include the pancreas, gallbladder uterus, and smaller than they are ovaries, thyroid and testes. Yet smaller are the adrenal glands, parotids, submandibular glands and the parathyroids.
| structure | length | width
ant-post |
trv | weight | volume | other | comment |
| adrenal | 3-5cms | 8gms | |||||
| aorta | 3cms proximal
1.75cms distal |
||||||
| breasts | 30-500gms | ||||||
| bile duct | 5mm | CHD at level of right hepatic artery | |||||
| brain | 1400gms | 1000-15000mls | |||||
| cervix | 2.5cms | 5cms | 2.5cms | ||||
| colon | 150cms
5ft |
5cms | |||||
| duodenum | 25cms | ||||||
| esophagus | 25-30cms | 2cms | |||||
| fallopian tube | |||||||
| femur | |||||||
| gallbladder | 8-10cms | 3-4cms | 50-70mls | ||||
| heart | 12cms | 6 | 8-9cms | 230-340gms | |||
| IVC | |||||||
| kidney | 11.25cms | 5-7.5cms | 125-170gms | ||||
| liver | 12-15cms | 10-12.5cms | 20-22.5cms | 1200-1800gms | largest gland in the body accounting for 2% of body weight and aslo the largest abdominal organ | ||
| lungs | 24cms | 630gms right
570gms left 900-1200gms |
4200-6300mls | 40% to 50% of the weight is blood
the right lung is slightly heavier than the left lung |
|||
| lymph node | <1cms | ||||||
| ovary | 2.5-5cms | 1.5-3cms | 1.5-3cms | 3-18mls | |||
| pancreas | 12-15cms | 1.5-3cms | 60-100gms | ||||
| pancreatic duct | 1-3mms | ||||||
| parathyroid | |||||||
| pituitary | 8-9mms | ||||||
| prostate | |||||||
| pulmonary vein | |||||||
| pulmonary artery | |||||||
| spinal cord | |||||||
| spleen | 12cms | 7cms | 4cms | 80-300gms | 250-350mls | ||
| small bowel | 700cms
23feet |
2.5cms | |||||
| stomach | |||||||
| thyroid | 4-6cms | 1-2cms | 2-3cms | 10-20gms | |||
| testis | 5cms | 3cms | 2cms | 15-20ccs | |||
| trachea | 2cms | ||||||
| ureter | 25-30cms | ||||||
| urethra | 4cms F
17-20cms M |
6mms | |||||
| urinary bladder | 12cms | 250 – 500mls | |||||
| uterus | 5-8cms | 1.5-3cms | 2.5-5cms | ||||
| vein | |||||||
Fom Freitas RA Junior Nanomedicine Volume 1 Basic Capabilities
Philip B. Hawk, Bernard L. Oser, William H. Summerson, Practical Physiological Chemistry, 12th Edition, The Blakiston Company, New York NY, 1951.
Peter L. Williams, Roger Warwick, Mary Dyson, Lawrence H. Bannister, eds., Gray’s Anatomy, Thirty-Seventh Edition, Churchill Livingstone, New York, 1989.
International Commission on Radiation Protection, Committee II, 1959, “Permissible Dose for Internal Radiation,” Health Phys. 3(1960):1.
Ivan Damjanov, James Linder, Anderson’s Pathology, Tenth Edition, Mosby, St. Louis MO, 1996.
capillaries which average 8 microns in diameter but may be as small as 4 microns –
red blood cells (7.8 micron x 2.6 micron biconcave disks) must fold in half to pass, single-file.
average animal cell is 10 -20 microns
human hair is about 80 microns
human eye can see up to 50 microns
sperm 60 X 5 nm
bacteria are as small as 1 micron
E Coli = 2micrometers long
ribosome 25nm diameter
cell membrane = 7.5-10nm thick
DNA molecule is about 2nanometers thick (nano = 1 billionth of a meter)
hydrogen atom = .1nanometer in diameter
0.1 nm (nanometer) diameter of a hydrogen atom
0.8 nm Amino Acid
2 nm Diameter of a DNA Alpha helix
4 nm Globular Protein
6 nm microfilaments
10 nm thickness cell membranes
11 nm Ribosome
25 nm Microtubule
50 nm Nuclear pore
100 nm Large Virus
150-250 nm small bacteria such as Mycoplasma
200 nm Centriole
200 nm (200 to 500 nm) Lysosomes
200 nm (200 to 500 nm) Peroxisomes
800 nm giant virus Mimivirus
1 µm (micrometer)
(1 – 10 µm) the general sizes for Prokaryotes
1 µm Diameter of human nerve cell process
2 µm E.coli – a bacterium
3 µm Mitochondrion
5 µm length of chloroplast
6 µm (3 – 10 micrometers) the Nucleus
9 µm Human red blood cell
10 µm
(10 – 30 µm) Most Eukaryotic animal cells
(10 – 100 µm) Most Eukaryotic plant cells
90 µm small Amoeba
100 µm Human Egg
up to 160 µm Megakaryocyte
up to 500 µm giant bacterium Thiomargarita
up to 800 µm large Amoeba
1 mm (1 millimeter, 1/10th cm)
1 mm Diameter of the squid giant nerve cell
up to 40mm Diameter of giant amoeba Gromia Sphaerica
120 mm Diameter of an ostrich egg (a dinosaur egg was much larger)
3 meters Length of a nerve cell of giraffe’s neck
Reference Wikibooks
interactive relative sizes (Utah)
Principles
Linear Measurements Length Diameter Radius
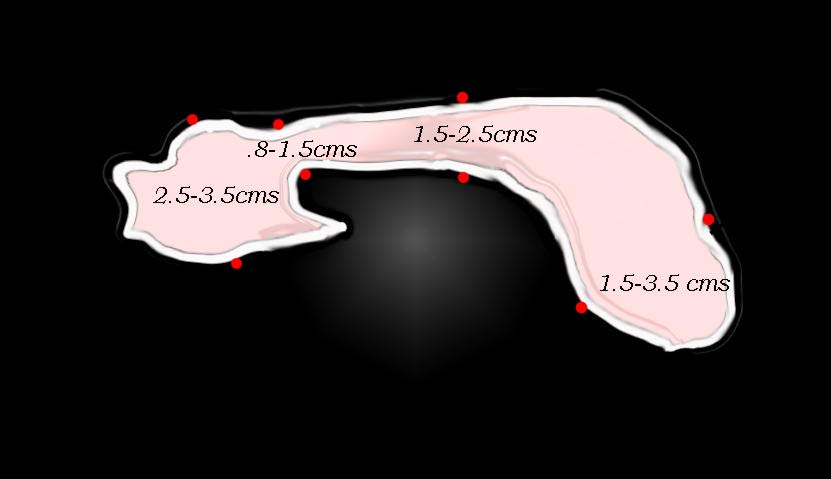
Size of the Pancreas |
| 41394size002b01 Courtesy Ashley Davidoff MD code pancreas size normal anatomy imaging drawing |
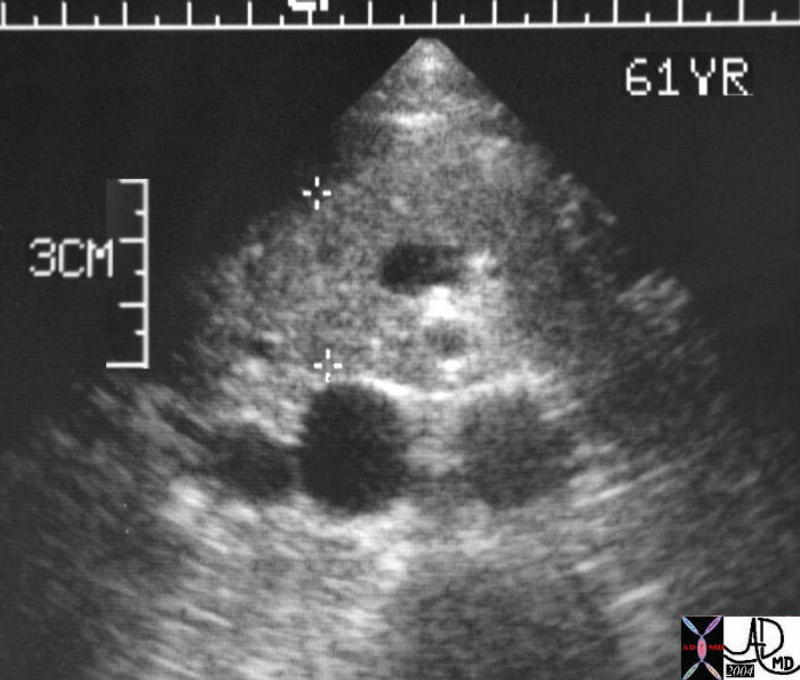
Head of the Pancreas |
| 39863b Courtesy Ashley Davidoff MD code pancreas 39k pancreatic head neck uncinate process fx normal dx normal anatomy size USscan |
Size and Pressure
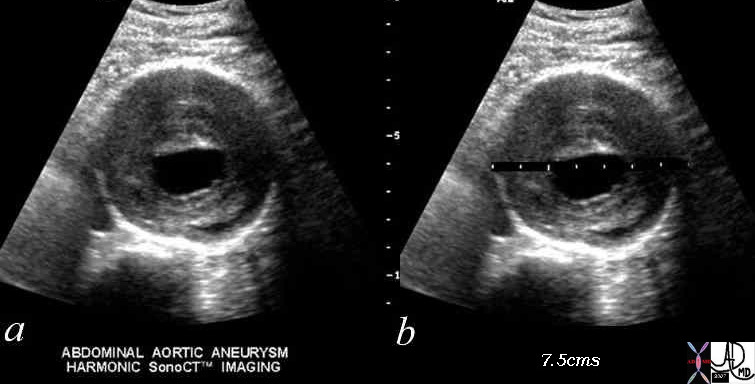
AAA 7.4cms – Indications for Surgical Intervention |
| 2055BH~1.c01 abdomen aorta abdominal aorta AAA aneurysm thrombus 7.5cms surgical size Courtesy Philips Medical Systems |
 
Normal and Ruptured Aorta |
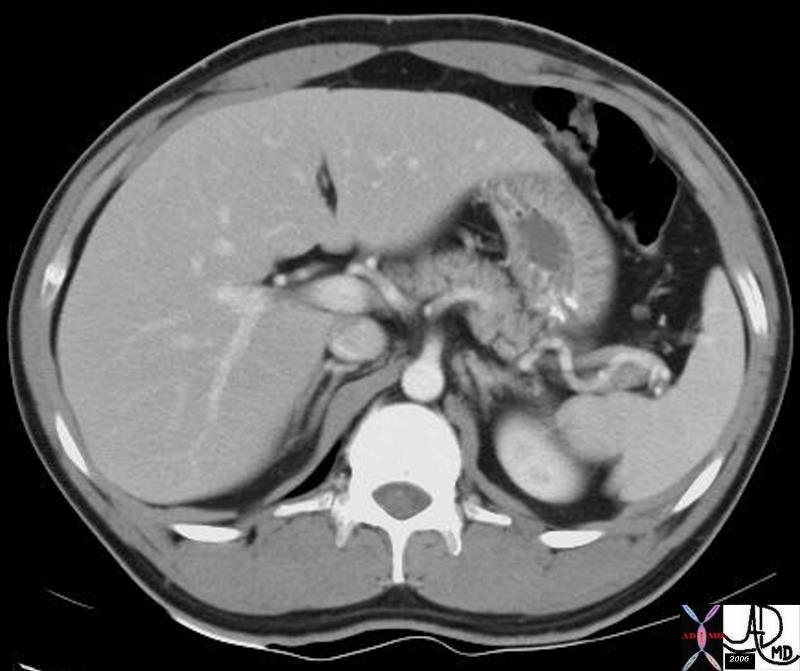
| 37004 abdomen aorta kidneys cortical phase subcurtaneous fat adipose tissue normal anatomy gallsones cholelthiasis CT scan Davidoff MD
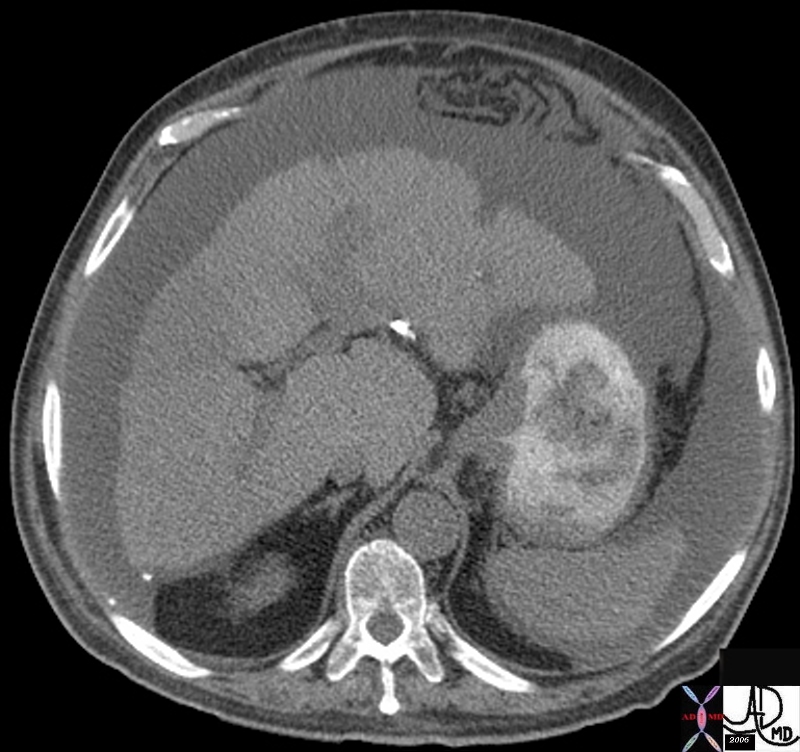
18269 aorta abdomen AAA aortic aneurysm abdominal aorta retroperitoneum fx retroperitoneal hematoma fx active hemorrhage fx perinephric hematoma anterior pararenal space perirenal space posterior pararenal space hemorrhage dx rupture abdominal aortic aneurysm CTscan Davidoff MD fx ruptured AAA |
Size and Time

Follicles in a Reproductive Female – Cyclical Phases -Size and Time |
| 71689 ovary follicles normal anatomy function physiology TCV Applied Biology Cycle time USscan Davidoff MD |
Size and Shape
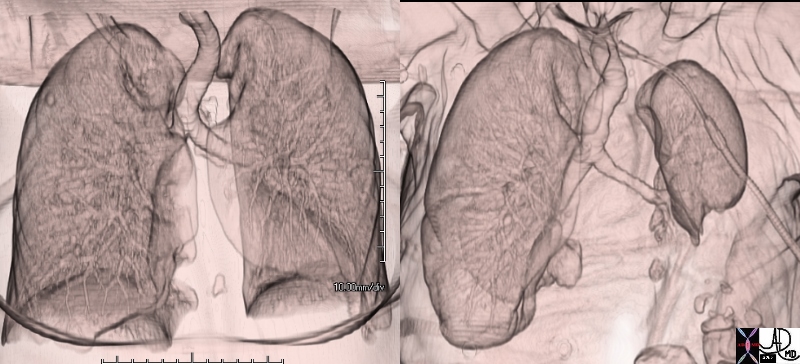
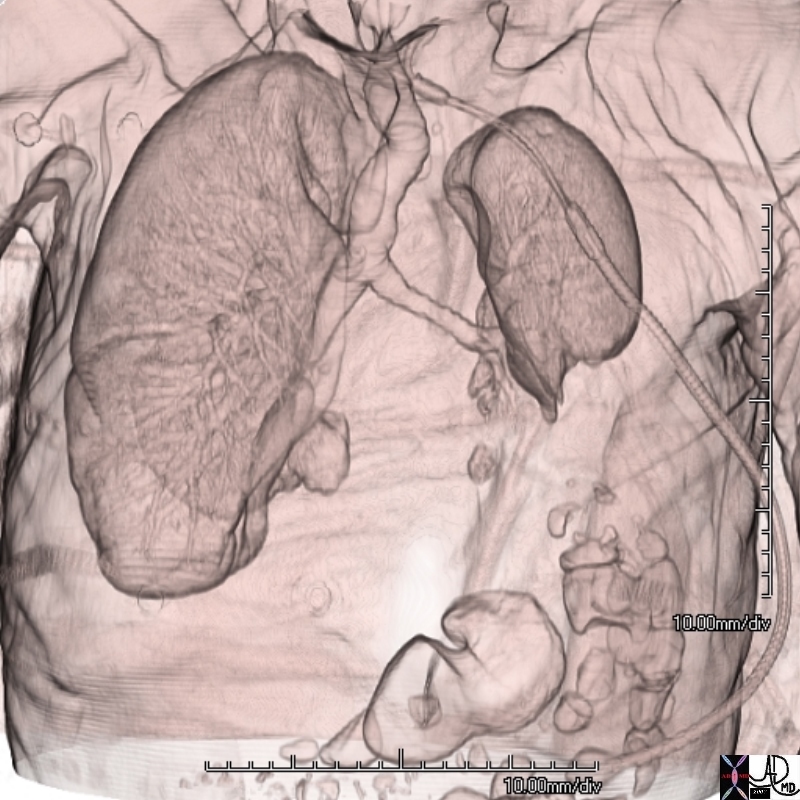
Normal vs Atelectasis |
| 74238c01 88 year old male bilateral complex effusions pleura pleural space atelecactasis space occupation normal 3D volume rendering CTscan Courtey Ashley DAvidoff MD |
Normal and Enlarged Abdomen |
| 45883.800 46133b03 abdomen skin size fx enlarged distended shape CTscan Cortesy Ashley Davidoff MD |
Relative Sizes
Relative Lengths |
| 34769c08 heart cardiac aortic valve pulmonary valve conus infundibulum RVOT right ventricular outflow tract pulmonary artery normal size aorta to PA ratio aorta to LA ratio anatomy CTscan Davidoff MD |
Relative Size of Bronchus and Pulmonary Artery |
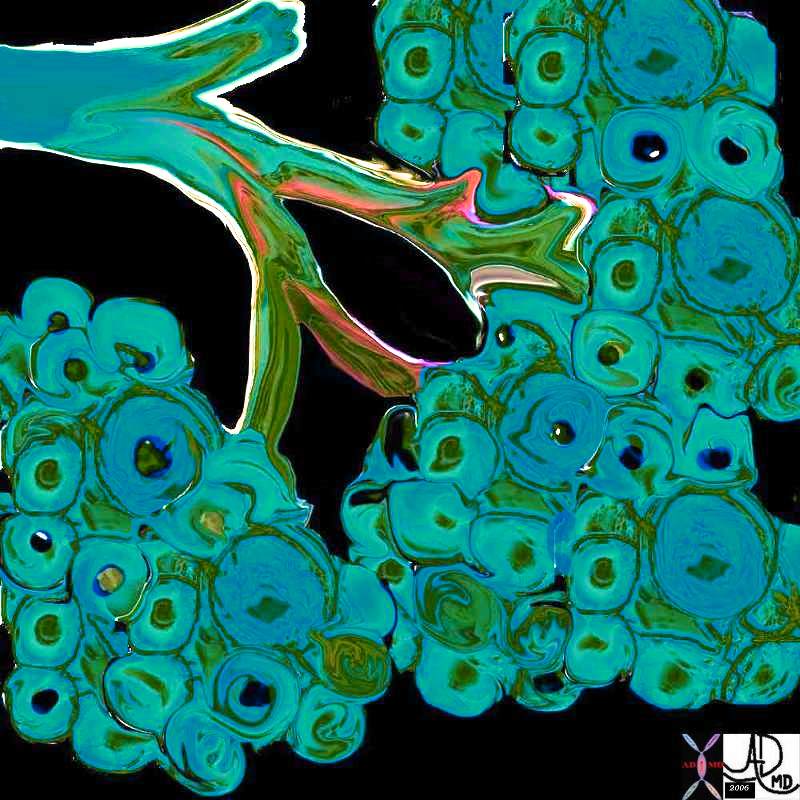
| 42464b07 In this normal CXR a RUL segmental bronchus and artery are side by side with the lucent air filled bronchus in teal and the artery in royal blue. Note that at his stage they are the same size and they will be for many divisions until they reach the terminal bronchiole. Courtesy Ashley Davidoff MD 42464b07 lung anatomy normal size applied biology applied anatomy |
Normal relationship and Size – Arterioles and Bronchioles |
|
In this CT of a normal patient we see two levels of the RLL with the segmental bronchioles and arterioles branching dichotomously and simultaneously. Note again the similarity in size and shape through these levels of division, a form that is maintained in the normal person until they reach the terminal bronchiole. 42455Courtesy Ashley Davidoff MD 42455 lung artery bronchus normal anatomy size applied anatomy applied biology |
 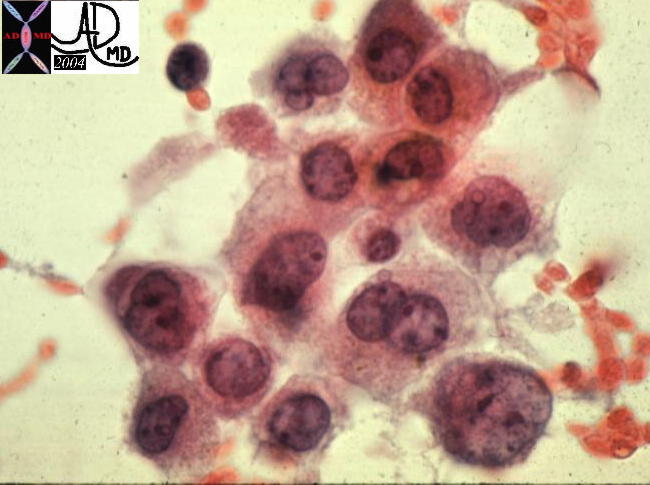
Which is the normal? The Nuclear-Cytoplasmic Ratio |
|
Size of the cytoplasm and Size of the Nucleus (N-C ratio) 13440 liver hepatocytes cells cytology histology normal 5star Courtesy Barbara Banner MD 13447 liver HCC hepatocellular carcinoma cytopathology Courtesy Barbara Banner MD |
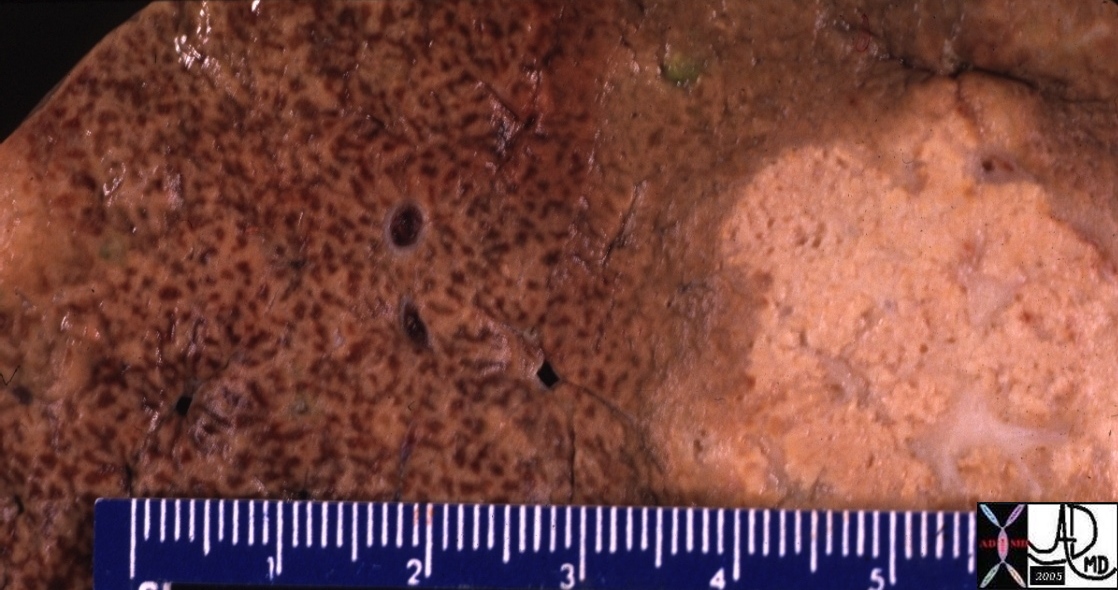
Length in Pathology – Nutmeg Liver |
| 00414 metastasis liver fx nutmeg liver hepatic congestion dx chronic passive congestion CHF congestive heart failure grosspathology Courtesy Ashley Davidoff MD |
Thickening
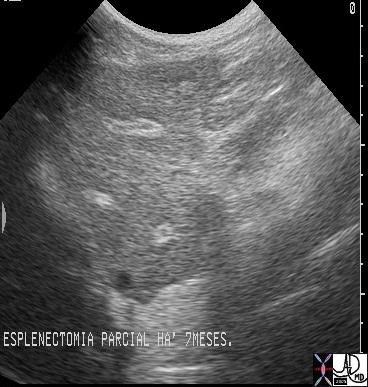
Schistosomiasis of the Liver – Thickened Periportal Tracts |
| 25170 liver vein portal fx periportal thickening dx schistosomiasis schistosoma Mansonii USscan |
Complex Pleural Effusion Thickened Pleura Chronic Inflammation Dystrophic Calcification |
| 74243b01 74242 74242b01 88 year old male complex effusions pleura pleural space thickened pleura thickening unilateral atelecactasis pleural calcification calcified CTscan Courtey Ashley DAvidoff MD |
Single versus Multiple
|
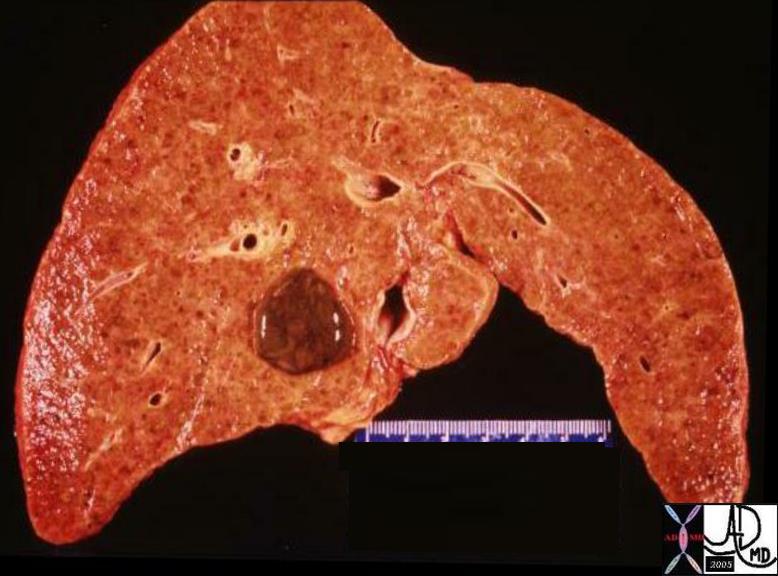
Single lesion vs Multiple Lesions |
| 03271 Hemorrhagic primary HCC 13448b01 liver hepatic metastases metastasis primary breast carcinoma biliary staining due tooc compression grosspathology TCV the common vein Davidof MD |

|
Single lesion vs Multiple Lesions |
| 02721 colon metastasis HCC 15764 liver hepatic metastases metastasis primary breast carcinoma Davidoff MD |

Volume Frequency
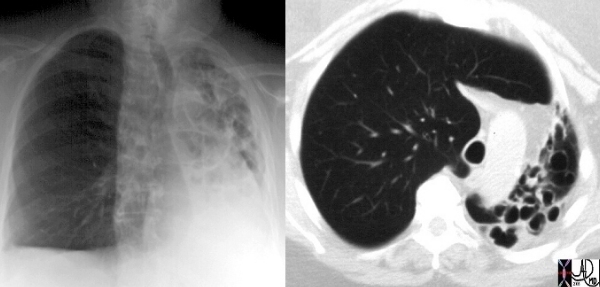
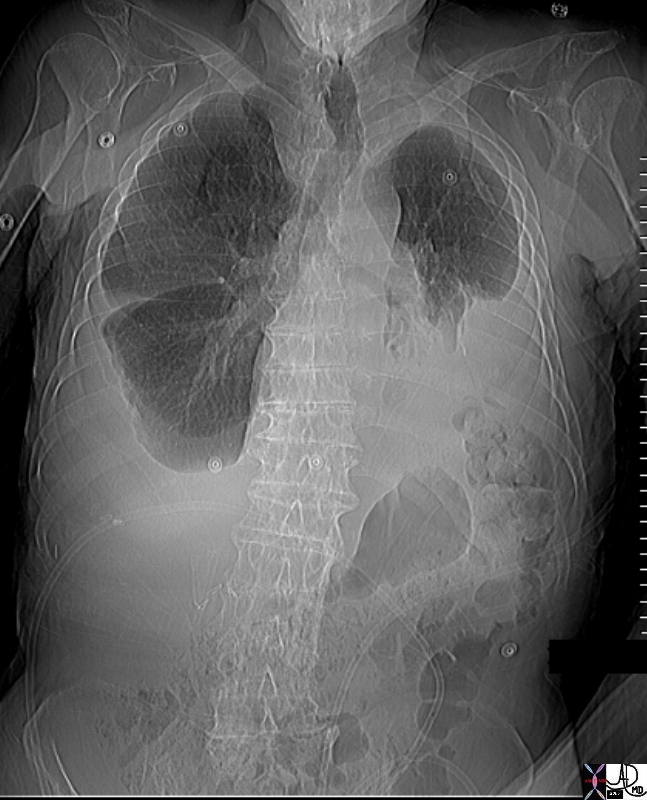
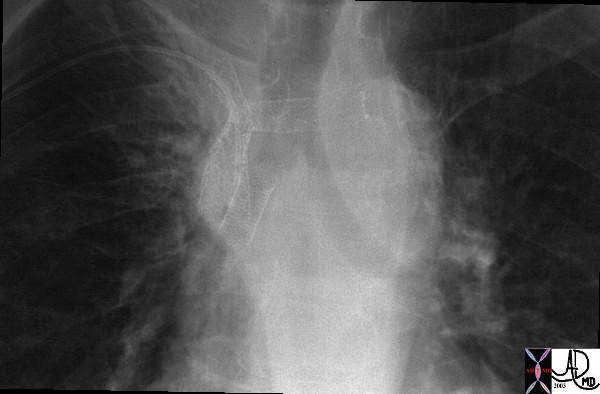
Volume Loss on Left and Hyperinflation on the Right |
| This image is a combination of a plain film showing a hyperinflated and large right lung, with volume loss and cystic change in the left lung. Note the proximal trachea is pulled to the left by the contracted left lung, as welll as pushed by the hyperinflated right lung. Courtesy Ashley Davidoff MD. code lung pulmonary trachea mediastinum bronchioles pushed pulled deviated shifted hyperinflated dilated cotracted emphysema bronchiectasis imaging radiology CTscan CXR palin film chest X-ray |
Volume Loss Due to Atelectasis and Effusion |
| 74242b01 88 year old male emaciated thin 3D volume rendering CTscan Courtey Ashley DAvidoff MD |
Volume
Volume Frequency
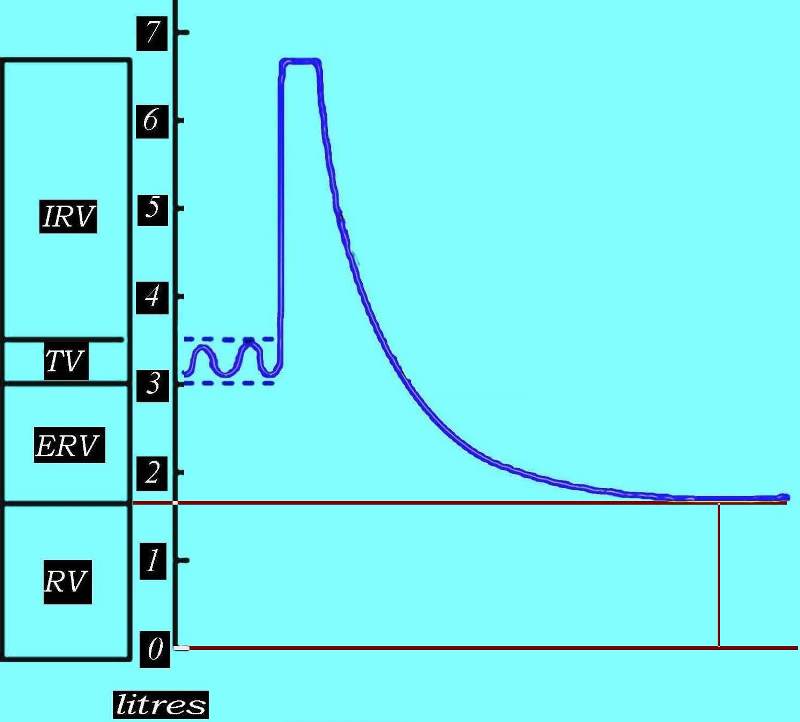
Volume Frequency |
| This diagram outlines the residual volume between the red lines, representing the air that is left in the airways and the alveoli after a full expiration. The air you may see on expiration CXR is the residual volume and as you can see it is about 1.8 liters in this patient.
Courtesy Ashley Davidoff MD. 42529b06aa03 |
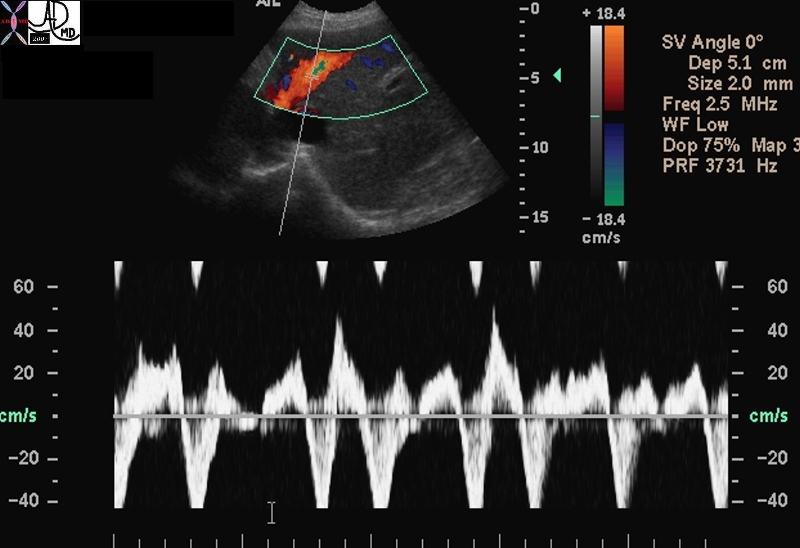
Flow Velocity |
| 70294 acv waves hepatic veins doppler tricuspid valve regurgitation TR velocity Ultrasound Echocardiogram Davidoff MD |
Weight

Weight |
| 02300p.800 scale weight size anatomy structure applied biology Davidoff photography |
 
A Single Abnormal Gigantic Floret – Gigantism a Quirk of Nature Variations in Size in Humans |
| 61229p flower allium size large elongated greater than the 90th percentile abnormally enlarged Davidoff photography
Former Olympian Olga Korbut (C) stands between Manute Bol (L) and William “The Refrigerator” Perry (R) during the weigh-in for Celebrity Boxing 2 in Los Angeles, California Tuesday, May 14, 2002. Korbut will face Darva Conger and Bol will face Perry during the boxing event which will air May 22 on Fox. REUTERS/John Hayes 54916.800 Olga 5feet 1 inch Manut Bol 7foot 7 inches William Perry 6’2” 370lbs |
By Body Part
The Body
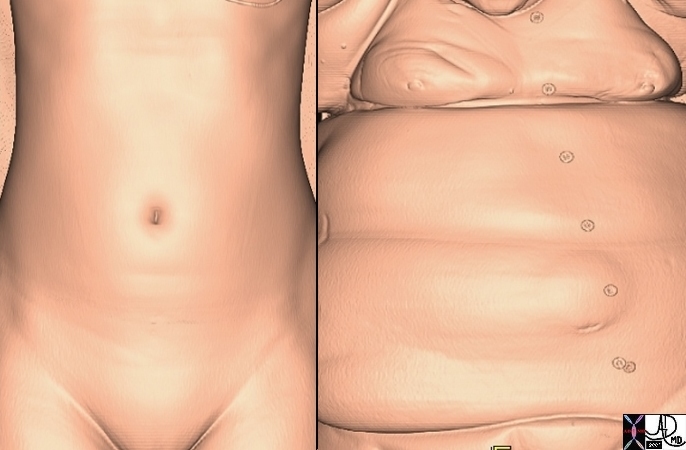
Body in Health and Disease |
| 49609c02 abdomen health disease normal obese morbid obesity order disorder Davidoff MD |
CNS
Size – Number
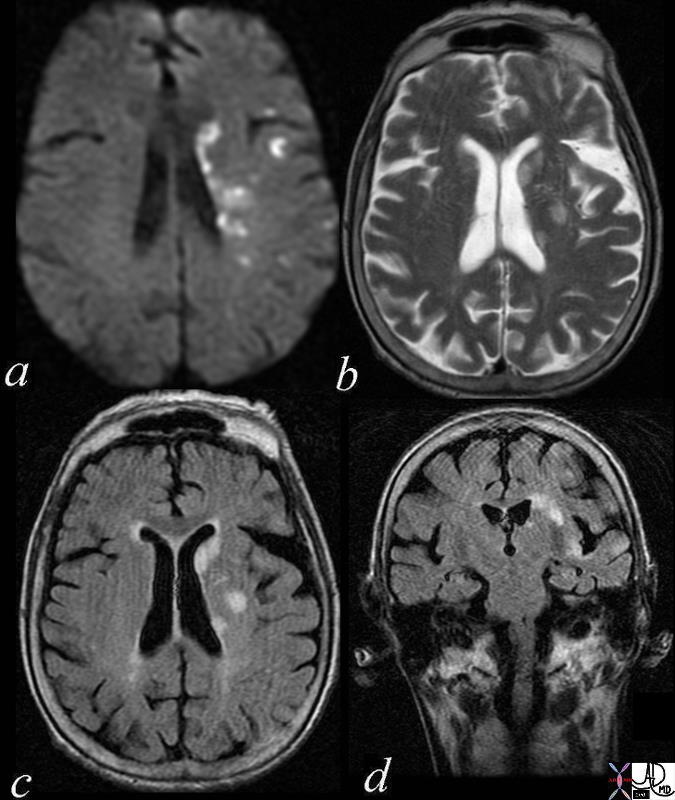
Multicentric Embolic Disease from Carotid Stenosis |
| 72014c01 brain cerebral multicentric infarcts internal capsule parietal lobe cortex dx multicentric infarct left cerebral hemisphere associated with a left carotid stenosis with presumed showering of the embolic material embolism a = DWI b = T2 weighted |
CVS
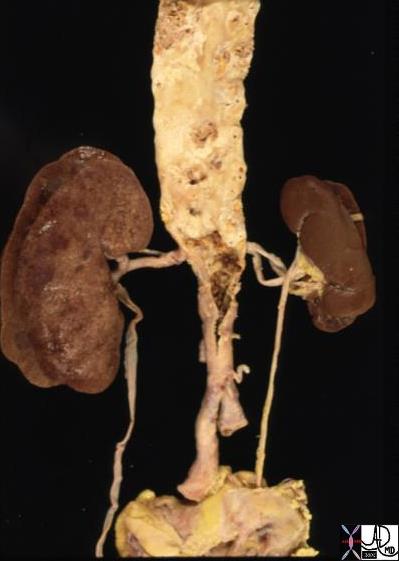
Relative Size – Small Left Kidney Normal to LArge Right Kidney |
| 13417 aorta abdomen iliac artery fx atherosclerosis kidney fx small dx RAS renal artery stenosis grosspathology Courtesy Ashley Davidoff MD |

Aortic Aneurysm |
| 42358.800 aorta fx enlarged MPA pulmonary artery aneurysm of the ascending aorta CTscan Davidoff MD |
Normal and AAA |
| 11976c01 aorta abdomen abdominal aorta renal afrteries kidney fx normal AAA abdominal aortic aneurysm horseshoe kidney angogram angiography lumbar arteries Davidoff MD |
Normal and Thickened Aortic Valve over Time |
| 07953c02 heart cardiac aorta aortic valve fx normal fx thickened fx bicuspid aortic valve fx calcified fx calcification fusion of the intercoronary commisures grossanatomy grosspathology Davidoff MD b Courtesy Henri Cuenoid MD |
Size Incompatible with Life
|
Mitral Atresia |
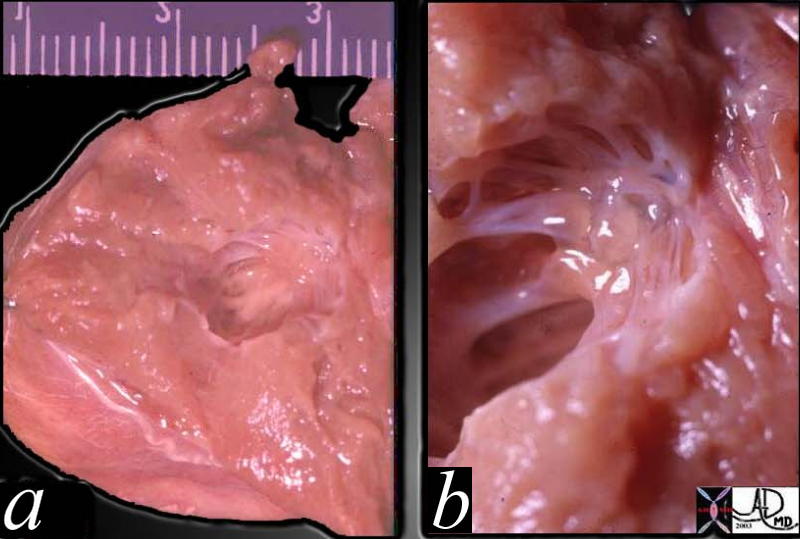
| This pathological image of the mitral valve is a close up of image 01810, showing an atretic MV with unformed and poorly formed elements including the chordae and papillary muscles. No lumen could be identified. The heart is incompatible with life
Courtesy Ashley Davidoff MD. 01813 (see 01810) code heart cardiac congenital grosspathology MV mitral atresia |

Normal Abdominal Aorta |
| This is an angiogram of a normal abdominal aorta. It consists of a suprarenal and an infrarenal component separated by the origin of the renal arteries. See image 24877d for color overlay. Courtesy Ashley Davidoff MD. 24877b |

| Infrarenal Abdominal Aortic Aneurysm |
| The digitally subtracted angiogram shows a fusiform infrarenal abdominal aortic aneurysm. There is mild ectasia of the right common iliac artery. Courtesy Ashley Davidoff MD 24590 |
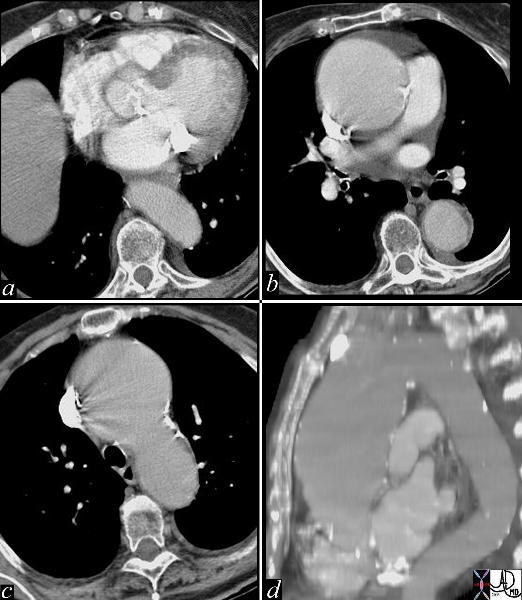
| Ascending Aortic Aneurysm |
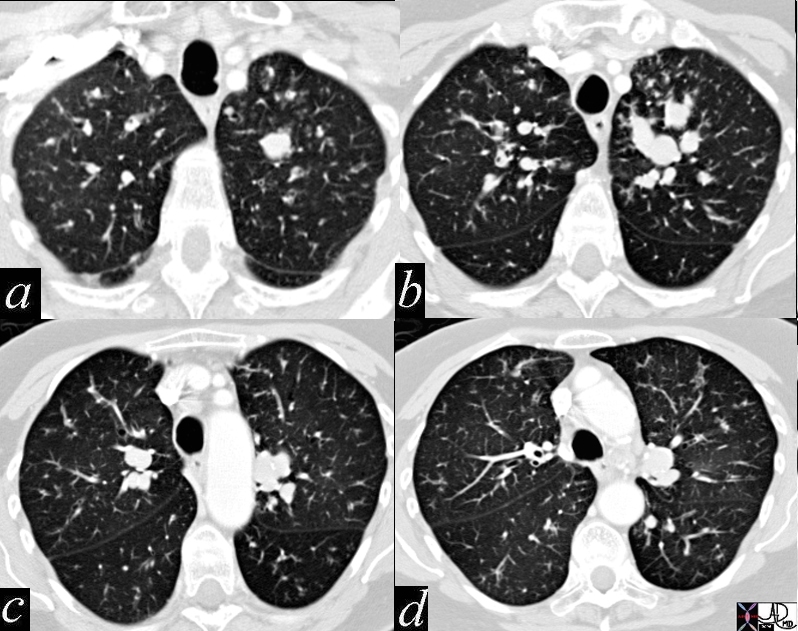
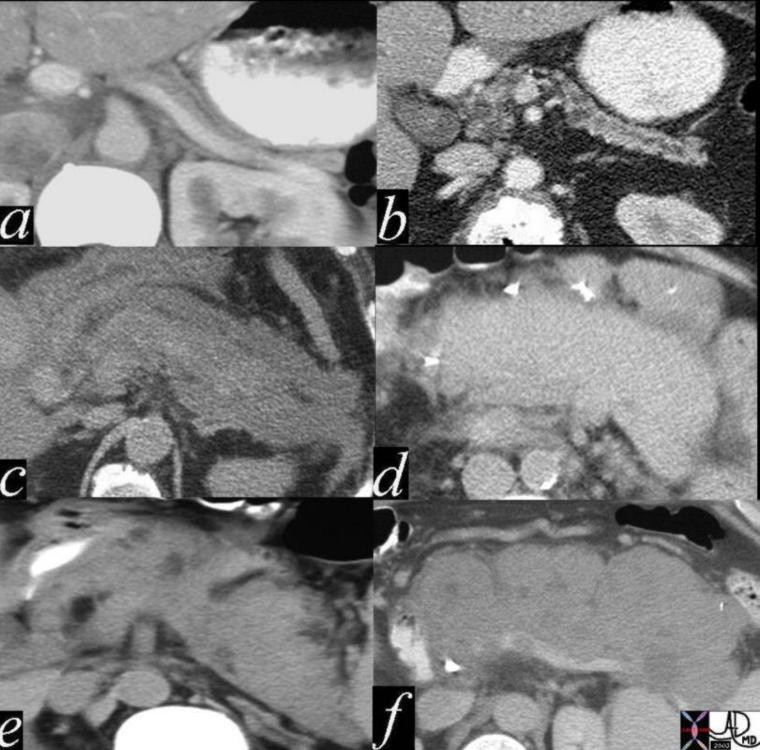
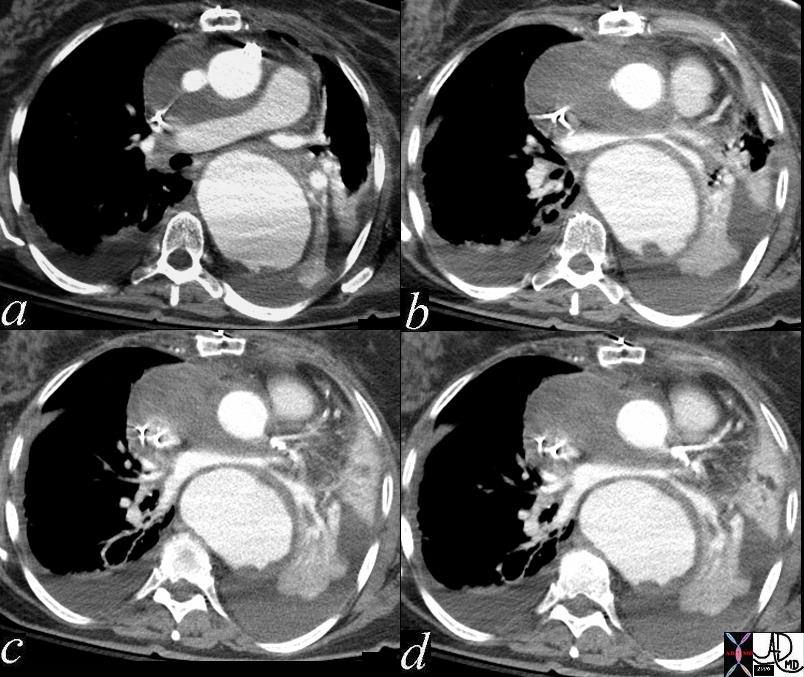
| This series of images are from a CTscan showing an ascending aortic thoracic aneurysm. There is evidence of heavy calcification of the aortic valve (aortic sclerosis), an aneurysm confined to the ascending aorta (b,c,d), and tortuosity of the descending aorta (d). The cause for the aneurysm is probably a combination of systemic hypertension, aortic stenosis and atherosclerotic degeneration of the wall. Courtesy Ashley Davidoff MD 19426c |
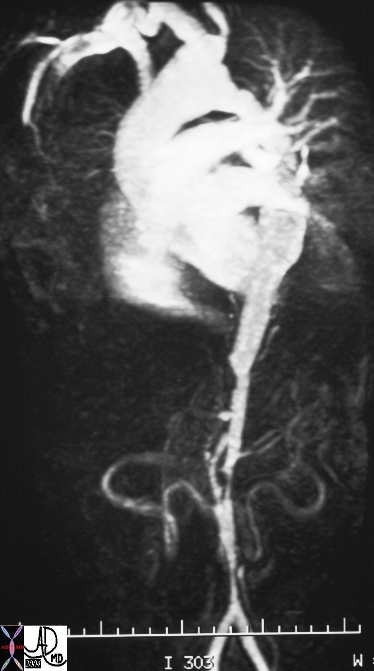
Multicentric and Diffuse Narrowing of the Abdominal Aorta |
| In this patient, the MRI shows narrowing of the abdominal aorta segmentally and diffusely in this patient who has Takayasu’s arteritis and aortitis – an inflammatory condition affecting the aorta and large arteries. 16917b Courtesy Ashley Davidoff MD |
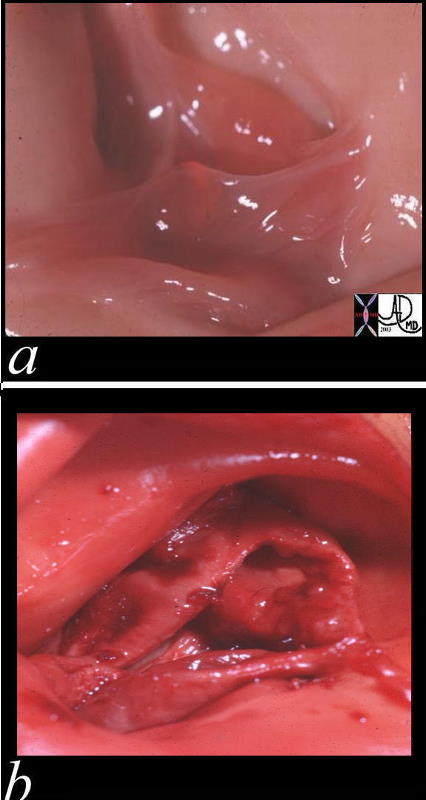
Normal and ongenitally Stenotic Pulmonary Valve |
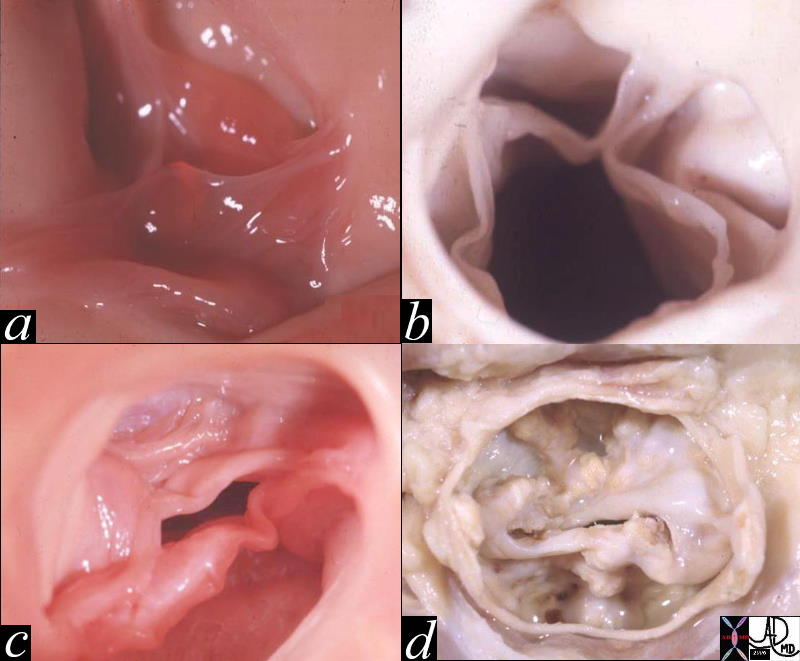
| These two pathological specimens of the pulmonary valve show the normal delicate leaflets of the normal valve (a) in comparison to the thickened leaflets of the bicuspid pulmonary valve Courtesy Ashley Davidoff MD 00272c01.800 |
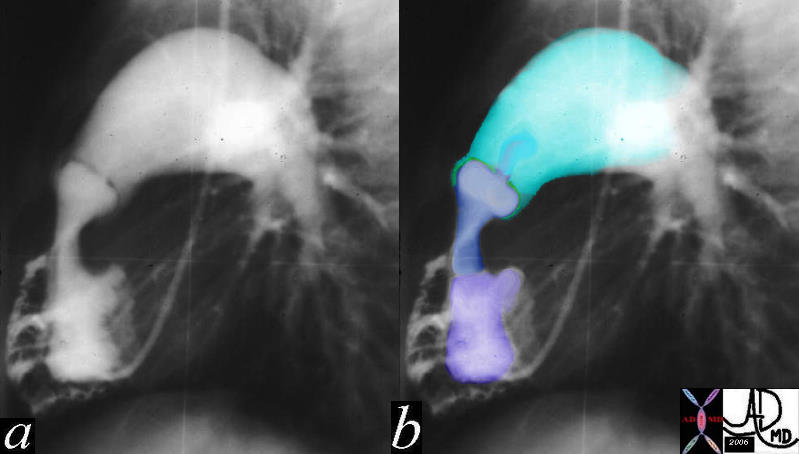
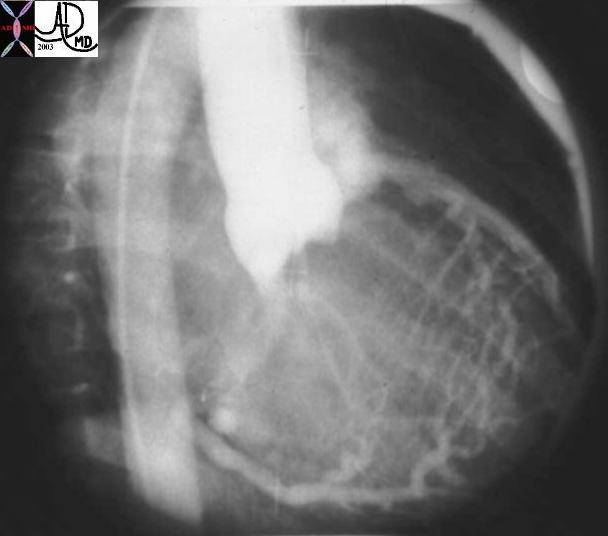
Severe Congenital Pulmonary Stenosis |
| The lateral projection of this right ventricular angiogram reveals a case of severe pulmonary stenosis. The catheter enters the RV from the RA via the SVC. The RV inflow tract (purple) is hypoplastic. The vessels emanating and theRV inflow are coronary arteries that are filling in retrograde fashion are due to the suprasystemic pressures in the RV indicating svere pulmonary stenosis with prssures in the RV that probably exceed 100mmhg. The infundibulum (right ventricular out flow tract (blue) is slightly narrow since it is hyperdynamic in an attempt to force the blood through the stenotic valve. The valve (green) is doming into the PA due the severe narrowing. The narrowing causes turbulence which causes the post stenotic dilatation.
15036c01 Courtesy Ashley Davidoff MD |
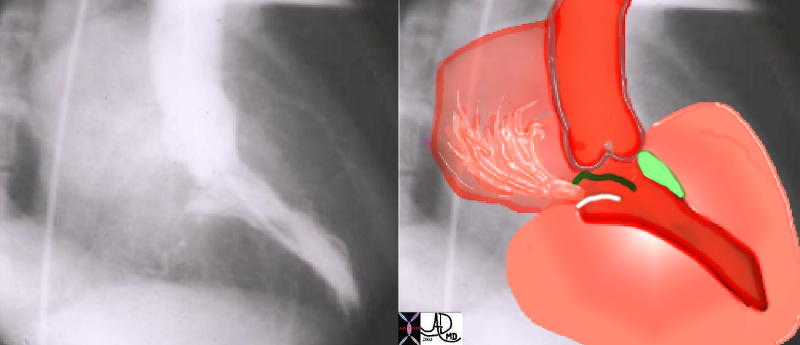
| Size and Shape – Play it again Sam |
| This angiogram in RAO projection shows a hypercontractile left ventricle that has a ballet shoe appearance, with mitral regurgitation filling the left atrium. The drawing shows the significant LVH small cavity of the LV, the area of subaortic muscle bundle (green) and the mitral regurgitation caused by the systolic anterior motion of the mitral valve. Courtesy Ashley Davidoff 34805 |
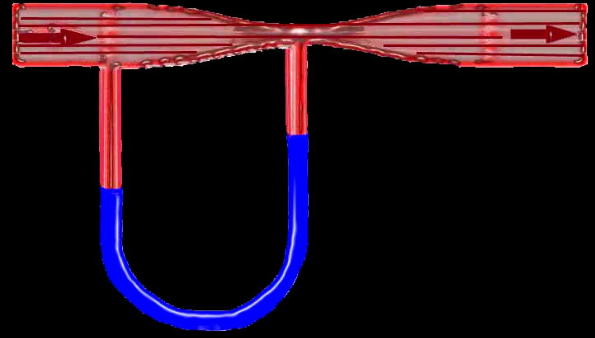
| Venturi – |
| Flow in this tube is demonstrated by the arrows going from right to left through a narrowingin the tube (red) demonstrating a vacuum or suction effect caused by the sudden acceleration of the fluid as it goes through the narrowing or stenosis. This is seen in the U shaped monometer with the fluid level in blue being relatively higher at the site of the stenosis in relation to the pressure more upstream. The suction phenomenon is kown as the Venturi effect is seen in IHSS where the narrowing of the LVOT causes a vacuum effect on the anterior leaflet of the MV resulting in mitral regurgitation. The Venturi effect is also utilised in the functioning of carburettors in fuel driven engines. 34807b05 |
Left Heart Failure |
| 46786c01 heart cardiac pulmonary arteries arteries fx enlarged fx corkscrew interstitial edema LAE left atrial enlargement dx cardiac failure cardiac congestion CTscan Davidoff MD |

Varicose Veins – Aging Body |
| Legs and feet seated at a bench in Quincy market in downtown Boston Massachusetts. – What story can you tell? Courtesy Ashley Davidoff MD. 02012p code foot accessory interesting vein varicose age time elderly shoe Davidoff photography |
| Size related to Volume and Pressure |
| This injection into the base of the aorta showing filling of a dilated right coronary artery, collateral flow through the septal perforators, into a dilated LAD and then into the main pulmonary artery. (MPA) This is a case of anomalous origin of the left coronary from the MPA. Courtesy Ashley Davidoff MD. 07024 |
RS
Normal Alveoli of the Lung and Emphysema |
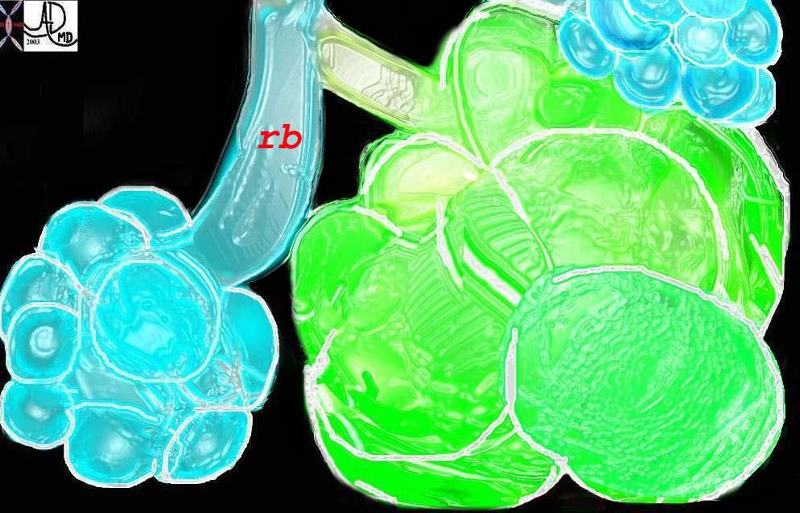
| This diagram illustrates the branching pattern of the tracheobronchial tree that extends from the bronchi to the terminal bronchioles transitioning into the alveoli via the alveolar sacs. Courtesy Ashley Davidoff MD 32645b04b04
This diagram shows alveoli and respiratory bronchioles that are too large due to loss of elasticity, so that air cannot be moved efficiently through them This is a diagram of emphysema causing hyperinflated lungs lung volumes 32645b01.800 Davidoff art |
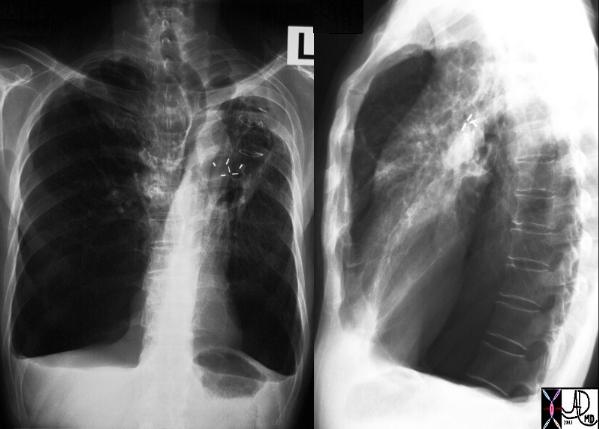
| Large lungs |
| A patient with hyperinflated lung volumes, COPD, and emphysema with surgical removal of a lung carcinoma from the LUL. Note how flattened the hemidiaphragms are and note the large retrosternal air space and the shapoe of the chest – like a barrel – called pectus carinatum – or pigeon chest. The lungs are literally so large that they are pushing the chest wall forward.
Courtesy Ashley Davidoff MD 30672c |
| CT of emphysema |
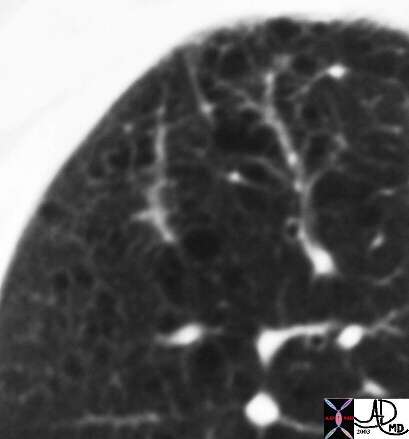
| This high resolution image of the lung shows “Swiss cheese” like black holes in the lung characterizing early cetrilobular emphysema in the right upper lobe. This degree of emphysema may be seen in a patient who has smoked and is in the their late 40’s or early fifties or in an elderly patient as an age related change in their 70’s or 80’s who has not smoked. Courtesy Ashley Davidoff MD. 01b 32170 |

| Segmental emphysema |
| This is a chest CT of a 29 year old man man who has segmental emphysema in the right lower lobe and midle lobe characterised by lucencies at 3 and 12 oclock where there has been air trapping in the alveoli. The left lung is normal This condition is called Swyer James syndrome Courtesy Ashley Davidoff MD. (30314 ) |

| Emphysema |
| This is an image of an emphysematous lung. Note the larger air spaces where the septae between the alveoli, alveolar sac, salveolar ducts and respiratory bronchioles have been broken down. 19932e |
Stenting the Obstructions |
| 0916030018 This is a case of a central squamous carcinoma causing obstruction of the right mainstem bronchus and SVC requiring stents in both. This image tells the story of how tubular transport function is compromised by reduced size, and how size can be restored by modern technology. 0916030018 Courtesy Ashley Davidoff MD size tracheobronchial tree SVC vein stent anatomy applied biology applied anatomy CXR |
Allergic Bronchopulmonary Aspergillosis |
| 47114c01 bronchi lungs fx dilated enlarged impacted with sft tissue finger in glove dx allergic bronchopulomonary aspergillosis ABPA aspergillus dx infection inflammation CTscan Davidoff MD |
Big Lung Small Lung Big Bronchi Small Bronchi |
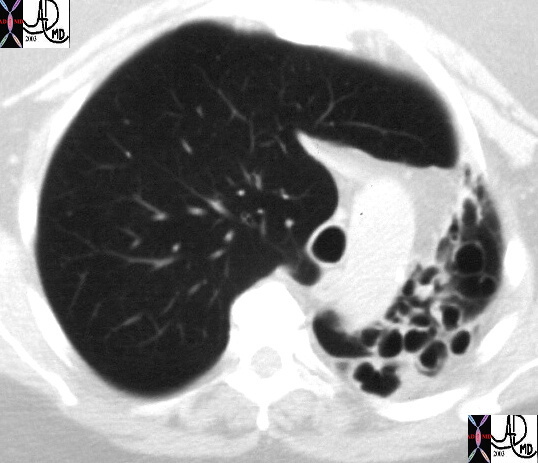
| This CT image shows a hyperinflated and large right lung, with volume loss and cystic change in the left lung. Note the trachea is pulled to the left by the contracted left lung, and is pushed by the hyperinflated right lung. Courtesy Ashley Davidoff MD. (30079 30084 30085 30085b) code lung pulmonary trachea mediastinum bronchioles pushed pulled deviated shifted hyperinflated dilated cotracted emphysema bronchiectasis imaging radiology CTscan |
GIT
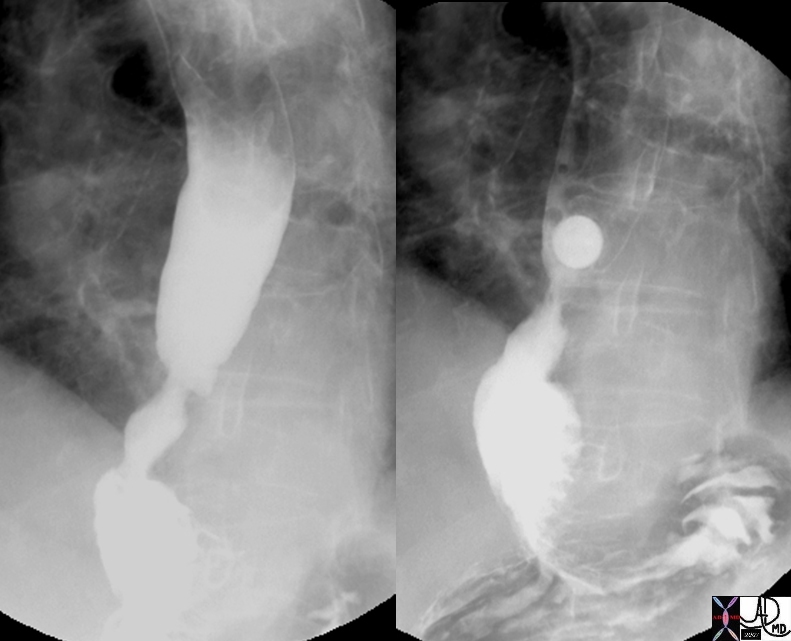
13 mm stricture in Esophagus |
| 49430c01 esopagus GE junction stricture hiatis hernia barium swsllow upper GI size Davidoff MD |
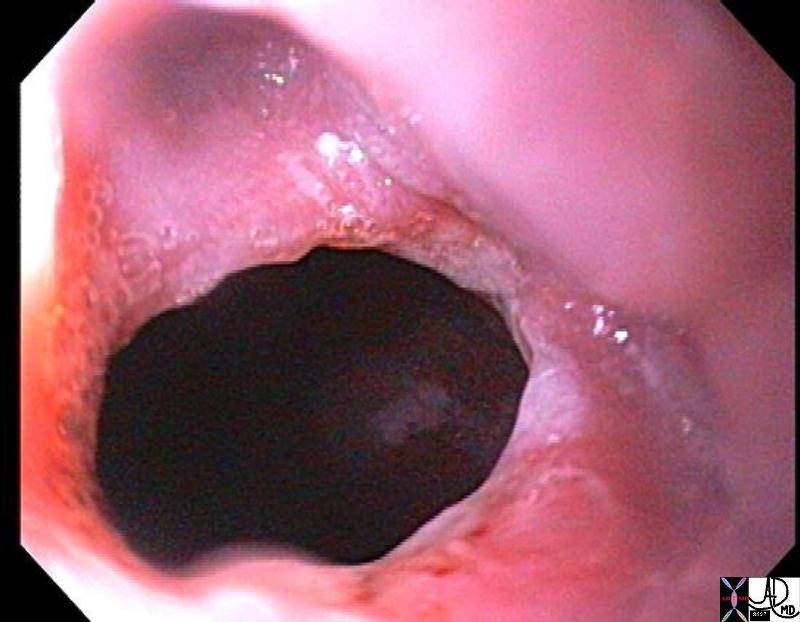
Stricture of the Esophagus |
| 73406.800 esophagus narrowing stenosis stricture distal esophageal stricture peptic stricture endoscopy Courtesy Joshua Namias |

Big Stomach |
| 17191 stomach gastric + fx dilated + enlarged gastrinoma + imaging radiology CTscan |

Big Stone |
| 00136 gallbladder stone large shadowing cholelithiasis imaging radiology USscan |

Small Stones – Cholecystitis |
| 00405 gallbladder multiple small dependant stones shadowing cholelithiasis gallbladder fossa fluid thickening acute cholecystitis positive Murphy’s sign imaging radiology USscan |
Small Pancreas Big Pancreas |
| 41394csize04 Courtesy Ashley Davidoff MD code pancreas size abnormal small enlarged anatomy imaging radiology CTscan |
Normal Liver and Cirrhosis |
|
Parts of the liver changing in size reflecting disease. The first image reflects a normal liver In the second image the left lobe is relatively large while the right lobe is small. These finding are characteristic of alcoholic cirrhosis. Note the shape of the surface of the liver has also changed from being smooth to being nodular and the presence of aciteds reflects a combination of increased portal pressure and low proteins. 18135.800 46136 Davidoff MD |
|
Normal Liver above Cirrhotic Liver below |
| This diagram reflects the large left lobe of the liver in cirrhosis and the small right lobe. The caudate lob is not depicted. 42649c01 Davidoff art |

GUT

Normal and Small – Kidneys |
| 46566c01 kidney kidneys size normal small anatomy physiology Davidoff MD |
|
Follicles in a Reproductive Female – Cyclical Phases -Size and Time |
| 71689 ovary follicles normal anatomy function physiology TCV Applied Biology Cycle time USscan Davidoff MD |
Sinle Kidney Bicornuate Uterus |
| 46527c01 uterus kidney renal bicornuate uterus single kidney congenital abnormality congenital growth disorder USscan MRI Davidoff MD |
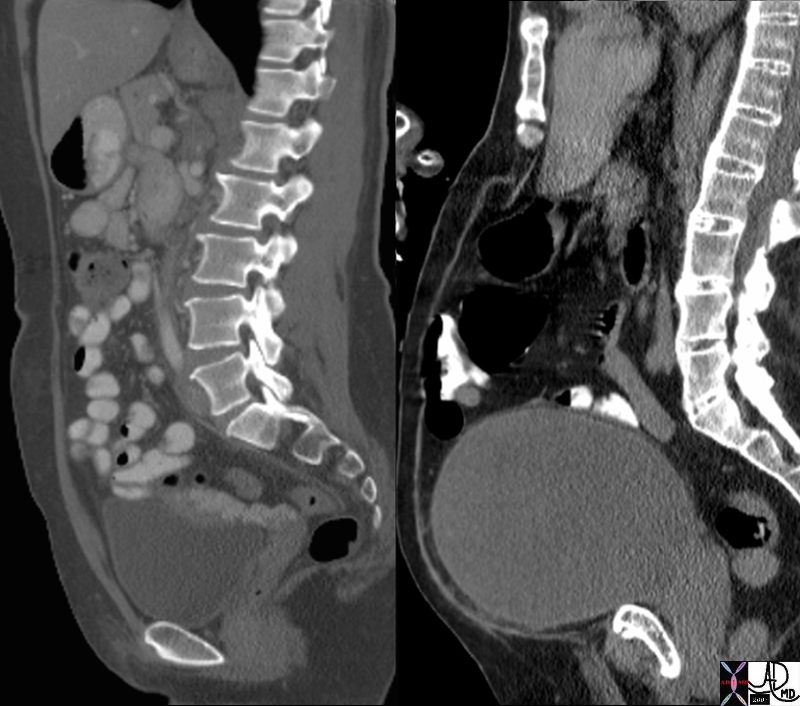
Normal Empty and Overdistended Symptomatic Full Urinary Bladder |
| 70363c09 urinary bladder normal enlarged abdominal pain induration abnormal urinary reterention CTscan sagittal reformat Davidoff MD |

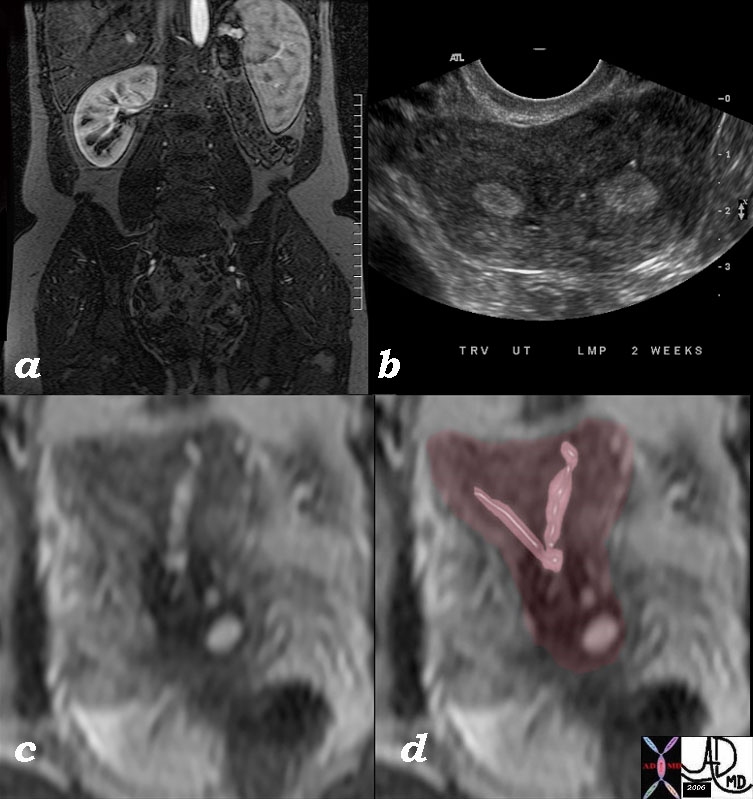
Hydrosalpinx |
| 43 old female with right adnexal discomfort and prior history of pelvic inflammatory disease Findings on a transvaginal ultrasound show a dilated fallopian tube consistent with hydrosalpinx
uterus fallopian tube distended hydrosalpinx ultrasound USscan 83331.8s Courtesy Ashley Davidoff MD copyright 2009 |
RES
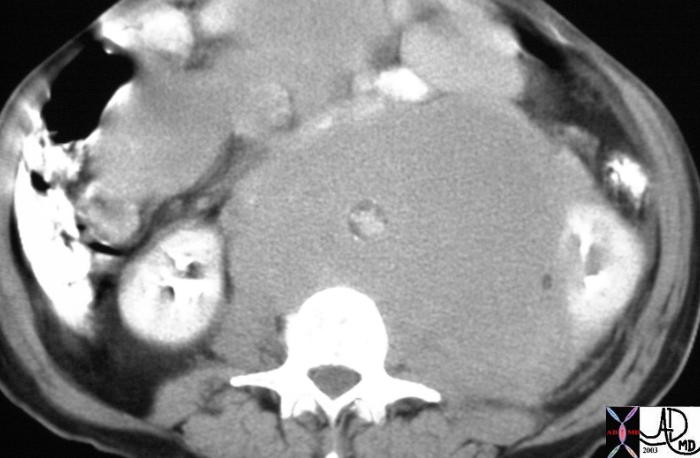
Big Lymph Nodes Small Aorta |
| This cross sectional image of the mid abdmen shows an aorta with an expanded diameter, which in this case is associated with an extremely small lumen. Note the wall of atherosclerotic calcification is on the inside of the soft tissue surrounding it. The case represents non-Hodgkins abdominal lymphoma that masquerades as an abdominal aortic aneurysm. The positioning of the calcification is key to this recognition. Courtesy Ashley Davidoff MD 15657 |
Skin
| Gynecomastia |
| 46621 hx 77 year old male with SOB breast pleura fx gynecomastia pleural calcification dx asbestos related disease dx asbestosis CTscan Davidoff MD 46621 46623 46624 46622 |
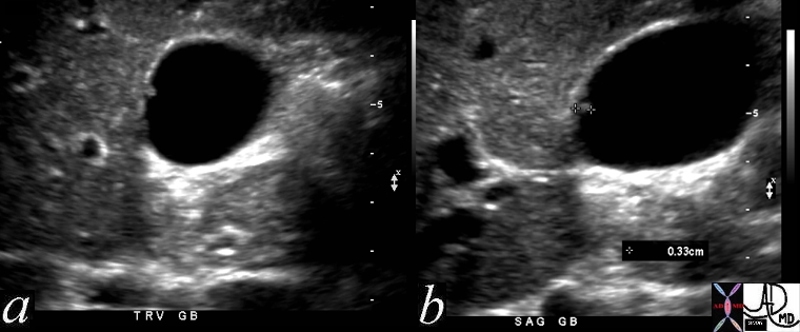
Gallbladder Polyp surrounded by fluid – 3mms |
| 47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD |
Varicose Veins in SVC syndrome |
| 38078 38078b01 this middle aged female with breast carcinoma skin veins pericardiophrenic veins pericardium pericardial fx collaterals varicocity varicose abdomen ascites dx SVC obstruction imaging radiology CTscan Courtesy Ashley Davidoff MD also code SVC syndrome |
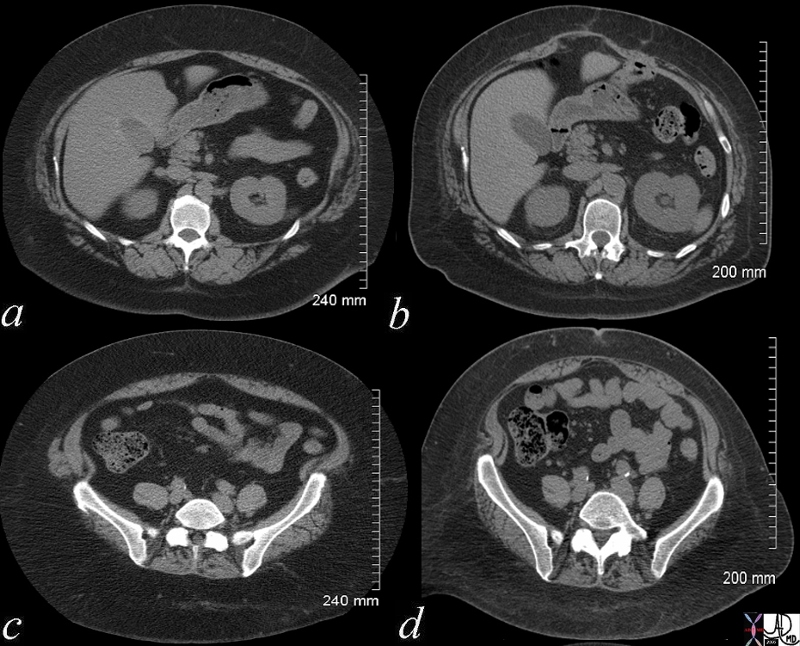
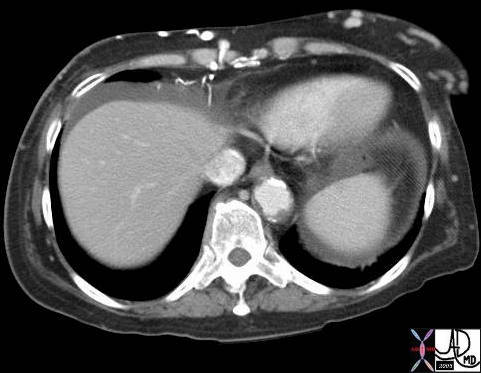
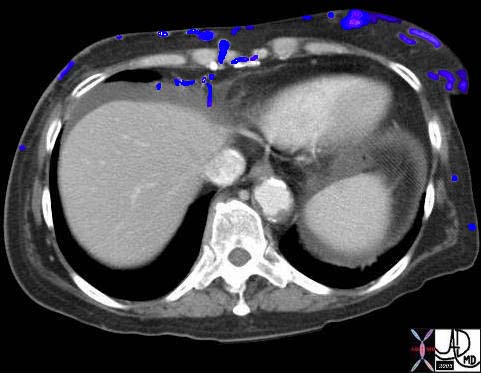
Obesity pre and post bypass |
| 48433c01.800 55 F s/p gastric bypass 4 years prior a, c pre bypass b,d post bypass adipose tissue subcutaneous fat size stomach nutrition metabolic fatty liver steatosis morbid obesity gallbladder fossa fatty sparing CTscan Courtesy Ashley Davidoff MD |
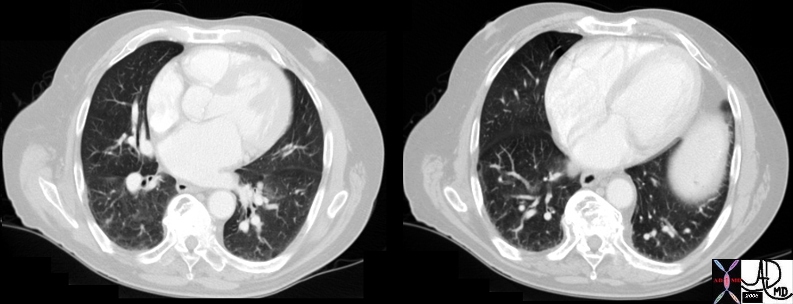
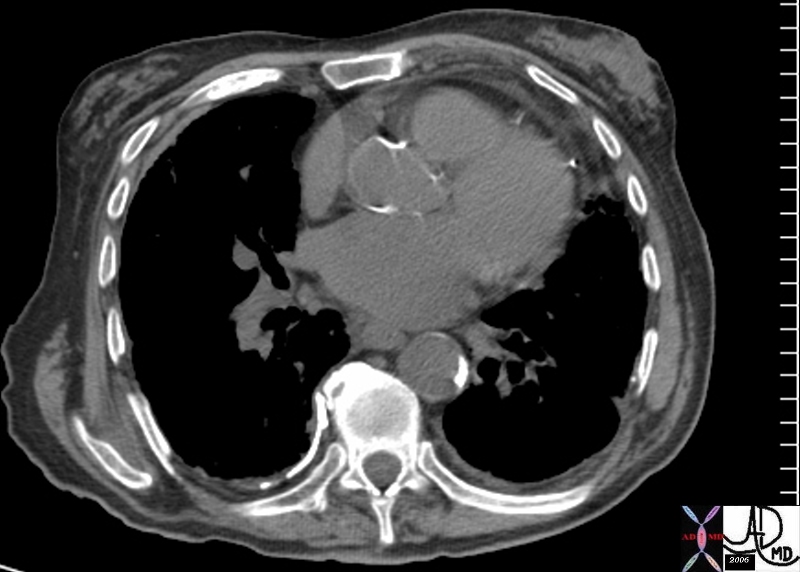
Large Abnormal Pushing and Squeezing |
|
61 year olsd female post op repair of ascending aortic aneurysm with Bental procedure with dropping blood pressure and odecreasing oxygen saturation aorta left atrium 47752c01 LA heart cardiacmediastinum fx compression of left atrium from anterior post operative nediastinal hematoma and posterior aneurysm of the descending aorta fx lingula atelectatasis and left lower lobe atelectasis bilateral pleural effusions dx supravalvular mitral stenosis CTscan Davidoff MD |
Size and Death |
| 46592c01 uterus OB pregnancy fetal demise spontaneous abortion shape size position heart rate USscan Davidoff MD death |
Size in Numbers
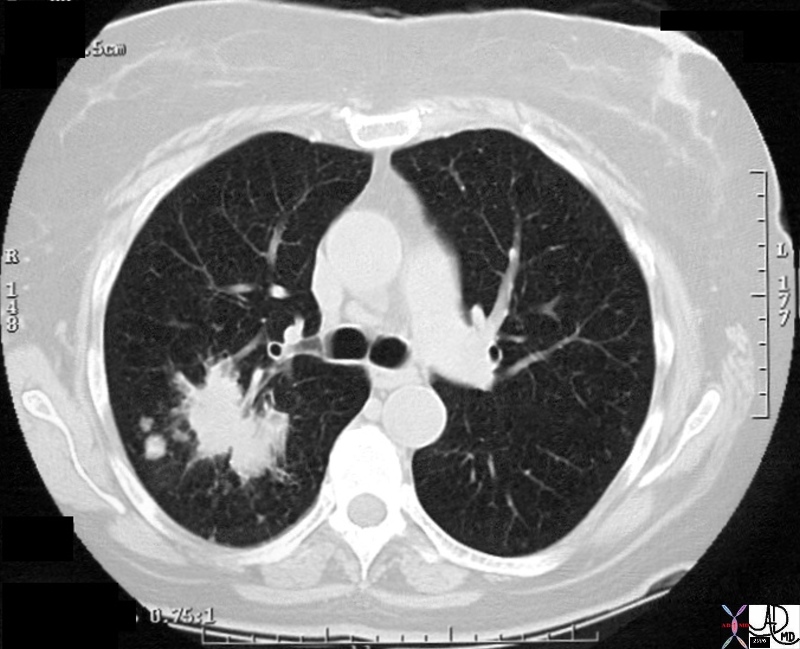
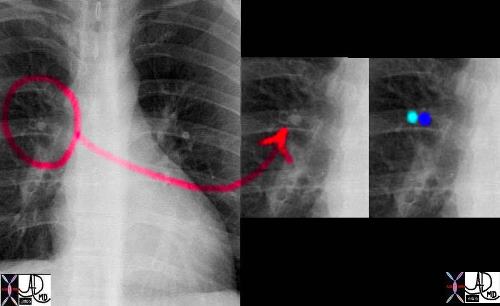
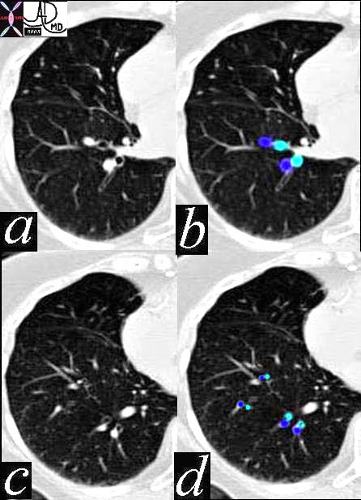
Satellite Nodules affect Staging of Cancer |
| 28980 chest lung spiculated mass satellite nodules malignant carcinoma CTscan Davidoff MD 28979 28980 28981 28984 28985 28986c01 |
Relative Sizes

Ascending Aortic Aneurysm |
| 42358.800 aorta fx enlarged MPA pulmonary artery aneurysm of the ascending aorta CTscan Davidoff MD |
Malignant Behaviour – Size and Doubling Time
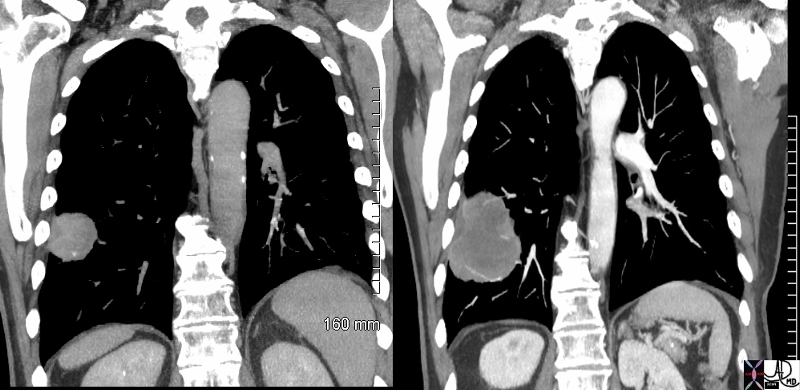
Growth of a lung lesion over 7 months |
| 48380c01 chest lung fx mass fx growth in 7 months dx metastattic squamous cell carcinoma head and neck primary primary larynx metastasis time size CTscan Davidoff MD 48383c01 48380c01 48383c02 malignant malignancy |
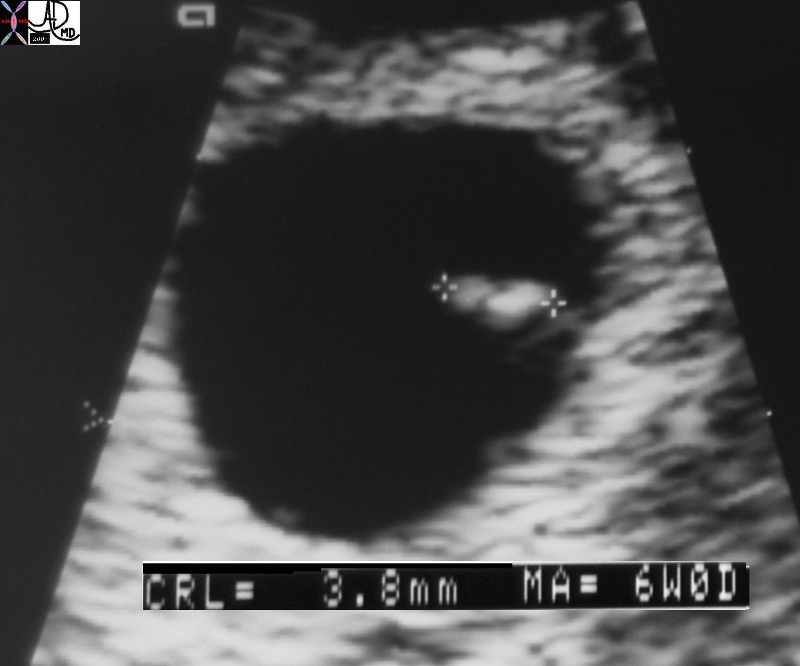
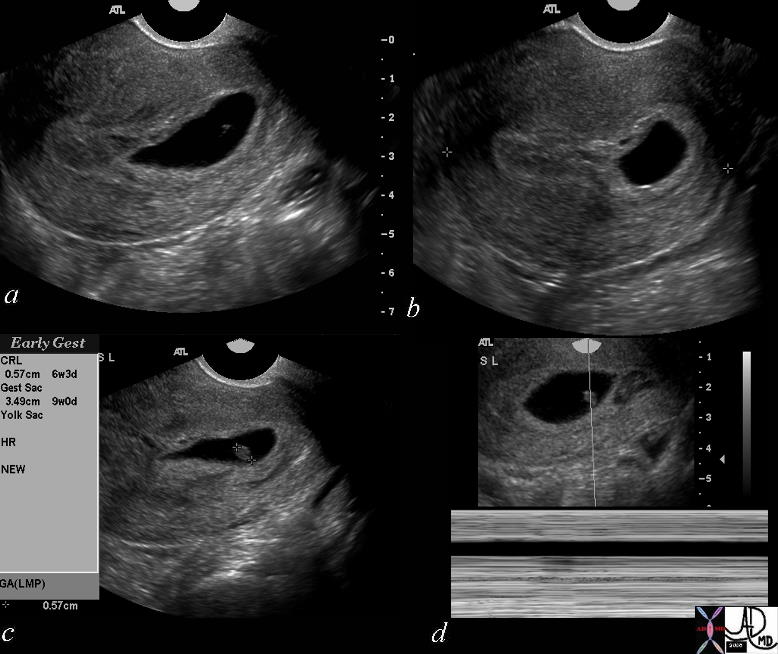
Size as Time – 3.8mm fetus – 6 weeks |
| 49786b01 fetal pole size dates time 6 weeks USscan obstetrics gestational sac amniotic cavity pregnancy Davidoff MD |

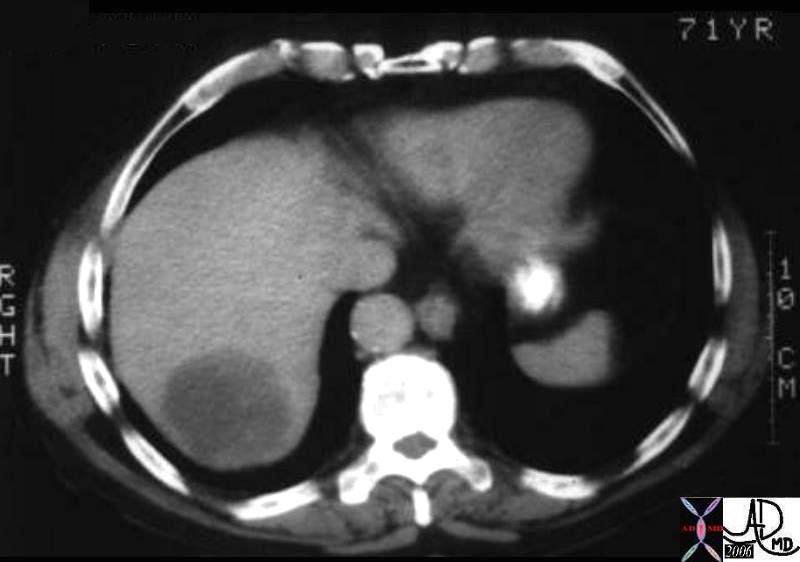
Chemotherapy – Before and 6 weeks After – Metastatic Small Cell Lung Carcinoma |
| 70248c01 liver metastattic small lung carcinoma with diffuse metatstattic disease to the liver )hepatic metastases metastasis before and after treatment 6weeks post chemotherapy successful result size change character change CTscan Davidoff MD 5star |
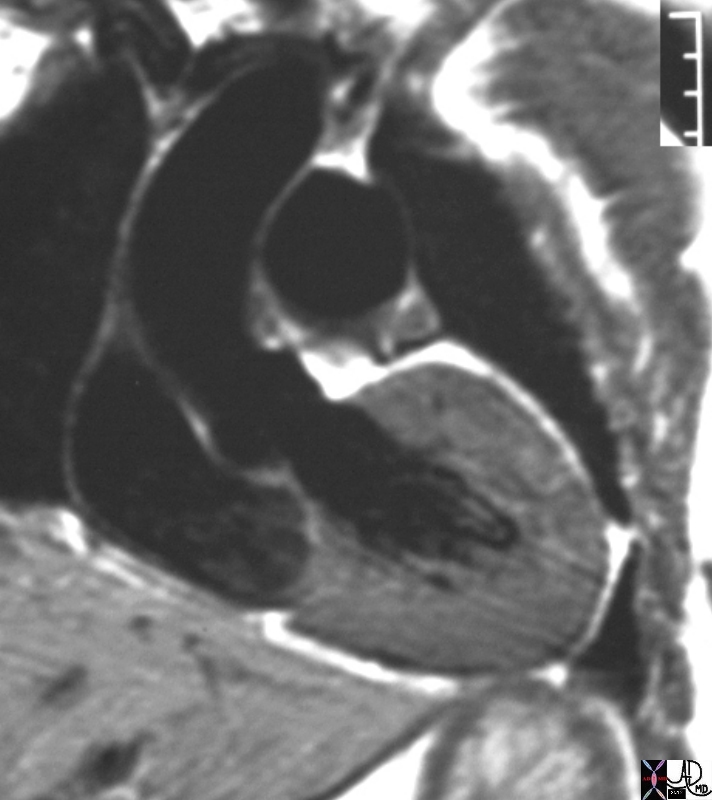
Left Ventricular Hypertrophy in a Patient with Coarctation of the Aorta |
| 16906.800 heart LV left ventricle aorta coarctation left ventricular hyperrophy fx LVH concentric hypertrophy dx coarctation imaging radiology T1 weighted MRI Courtesy Ashley Davidoff MD |
The concept of space may be taken even further in noting the size differential between the liver’s conduit vessels and its cells. The portal vein is typically 6-8 mm in diameter while each hepatocyte measures in microns. Besides the obvious conclusion that each hepatocyte occupies less space than the portal vein this size difference also indicates that each cell is much more limited in terms of the size of molecules and compounds that may be transported through it. This equates to (try and find an example in our surrounding life that will exemplify this difference).
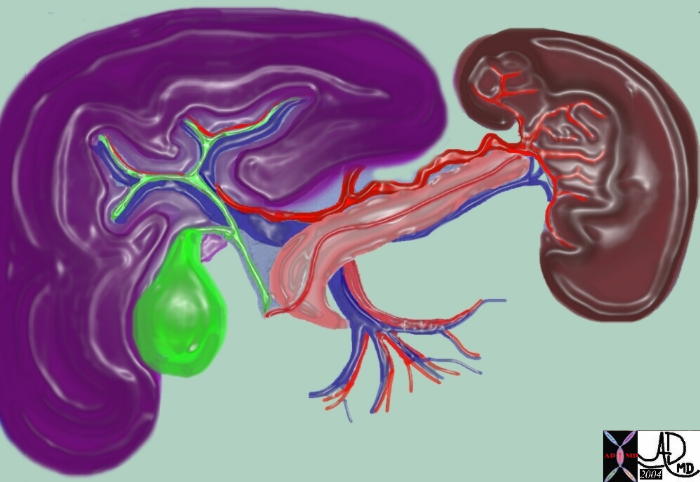
Porta Hepatis – Road of the Liver |
| 63288 C liver spleen pancreas gallbladder bile duct celiac axis portal triad hepatic duct portal vein hepatic artery normal anatomy Davidoff art |

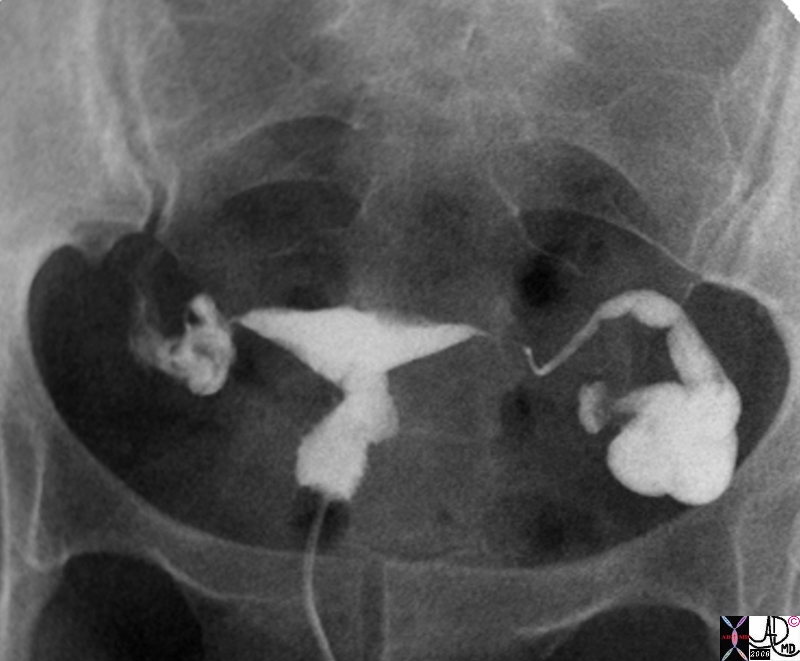
Obstructed Left Tube Hydrosalpinx |
| 33 old female with left adnexal discomfort and prior history of pelvic inflammatory disease Findings on hysterosalpingogram show a dilated fallopian tube consistent with hydrosalpinx uterus fallopian tube distended hydrosalpinx
83340b01.8s ultrasound USscan Courtesy Ashley Davidoff MD copyright 2009 |
As remarkable as the liver may be, let us not forget the centrality of space to the functioning of all of the body’s structures. It is also important to consider glands, which are spatially organized around blood vessels to optimally receive raw products and around ducts to optimally secrete their final products. Also not to be forgotten are the spatial relationships between nerve cells, whose synaptic clefts must remain within narrow parameters for the proper release and uptake of neurotransmitter. Even the heart’s ability to pump relies in part upon the spacing of its constituent cells, as cardiac muscle cells are closely packed in tight junctions to allow for the rapid propagation of action potentials through the atria and ventricles. Indeed, in these and many other ways the specific association of neighboring cells and tissues is what keeps each one of us alive.
Space is the position in which a biologic unit is found.
 
69798.800 |
| 69798.800 leaf tree branch parts tubes transport veins maple leaf Davidoff photography |
Spatial relationships between structures is critical to optimising function.